

#74 – Dr Greg Lewis on COVID-19 and reducing global catastrophic biological risks
#74 – Dr Greg Lewis on COVID-19 and reducing global catastrophic biological risks
By Howie Lempel, Robert Wiblin and Keiran Harris · Published April 17th, 2020
On this page:
- Introduction
- 1 Highlights
- 2 Articles, books, and other media discussed in the show
- 3 Transcript
- 3.1 Rob's intro [00:00:00]
- 3.2 The interview begins [00:03:15]
- 3.3 What is COVID-19? [00:16:05]
- 3.4 If you end up infected, how severe is it likely to be? [00:19:21]
- 3.5 How does COVID-19 compare to other diseases? [00:25:42]
- 3.6 Common confusions around COVID-19 [00:32:02]
- 3.7 What types of interventions were available to policymakers? [00:46:20]
- 3.8 Nonpharmaceutical Interventions [01:04:18]
- 3.9 What can you do personally? [01:18:25]
- 3.10 Reflections on the first few months of the pandemic [01:23:46]
- 3.11 Global catastrophic biological risks (GCBRs) [01:26:17]
- 3.12 Counterarguments to working on GCBRs [01:45:56]
- 3.13 How do GCBRs compare to other problems? [01:49:05]
- 3.14 Careers [01:59:50]
- 3.15 The response of the effective altruism community to COVID-19 [02:11:42]
- 3.16 The response of 80,000 Hours to COVID-19 [02:28:12]
- 3.17 Rob's outro [02:36:22]
- 4 Learn more
- 5 Related episodes
A painting illustrating the Black Death — the worse pandemic in human history, which killed 30-60% of Europe's population.



Our lives currently revolve around the global emergency of COVID-19; you’re probably reading this while confined to your house, as the death toll from the worst pandemic since 1918 continues to rise.
The question of how to tackle COVID-19 has been foremost in the minds of many, including here at 80,000 Hours.
Today’s guest, Dr Gregory Lewis, acting head of the Biosecurity Research Group at Oxford University’s Future of Humanity Institute, puts the crisis in context, explaining how COVID-19 compares to other diseases, pandemics of the past, and possible worse crises in the future.
COVID-19 is a vivid reminder that we are vulnerable to biological threats and underprepared to deal with them. We have been unable to suppress the spread of COVID-19 around the world and, tragically, global deaths will at least be in the hundreds of thousands.
How would we cope with a virus that was even more contagious and even more deadly? Greg’s work focuses on these risks — of outbreaks that threaten our entire future through an unrecoverable collapse of civilisation, or even the extinction of humanity.
If such a catastrophe were to occur, Greg believes it’s more likely to be caused by accidental or deliberate misuse of biotechnology than by a pathogen developed by nature.
There are a few direct causes for concern: humans now have the ability to produce some of the most dangerous diseases in history in the lab; technological progress may enable the creation of pathogens which are nastier than anything we see in nature; and most biotechnology has yet to even be conceived, so we can’t assume all the dangers will be familiar.
This is grim stuff, but it needn’t be paralysing. In the years following COVID-19, humanity may be inspired to better prepare for the existential risks of the next century: improving our science, updating our policy options, and enhancing our social cohesion.
COVID-19 is a tragedy of stunning proportions, and its immediate threat is undoubtedly worthy of significant resources.
But we will get through it; if a future biological catastrophe poses an existential risk, we may not get a second chance. It is therefore vital to learn every lesson we can from this pandemic, and provide our descendants with the security we wish for ourselves.
Today’s episode is the hosting debut of our Strategy Advisor, Howie Lempel.
80,000 Hours has focused on COVID-19 for the last few weeks and published over ten pieces about it, and a substantial benefit of this interview was to help inform our own views. As such, at times this episode may feel like eavesdropping on a private conversation, and it is likely to be of most interest to people primarily focused on making the long-term future go as well as possible.
In this episode, Howie and Greg cover:
- Reflections on the first few months of the pandemic
- Common confusions around COVID-19
- How COVID-19 compares to other diseases
- What types of interventions have been available to policymakers
- Arguments for and against working on global catastrophic biological risks (GCBRs)
- Why state actors would even use or develop biological weapons
- How to know if you’re a good fit to work on GCBRs
- The response of the effective altruism community, as well as 80,000 Hours in particular, to COVID-19
- And much more.
Get this episode by subscribing to our podcast on the world’s most pressing problems and how to solve them: type “80,000 Hours” into your podcasting app. Or read the transcript below.
Producer: Keiran Harris.
Audio mastering: Ben Cordell.
Transcriptions: Zakee Ulhaq.
Highlights
The thinking behind social distancing
A lot of the physical distancing recommendation you’re seeing from various governments, including my own in the UK, is essentially trying to act as an insurance against this risk of people spreading it to others without either person realizing they’re at risk. So, in a sense, this idea of like, avoid all non-essential contact with others, doesn’t have a rider of like, “Oh, if both of you feel well it’s fine,” partly for reasons like this. But also people may not always recollect what symptoms they have. If you’re coughing like once or twice a day or something, maybe that’s a sign of a very mild infection for argument’s sake. But you may not notice that, potentially, and think you’re well. And so given all these things, there’s this general urge towards just basically making as little in-person social contact as possible as a way of reducing the spread of the disease.
If you knew for sure that only people who were having symptoms could spread it, which may have been the case in SARS, although there’s slightly more of a story there, then maybe this wouldn’t be as necessary over and above a milder principle of, “Please isolate when you’re feeling unwell”. But unfortunately that doesn’t seem to be the case, and hence why we’re seeing what we’re seeing now.
Why will it take at least 12-18 months to get a vaccine?
It’s worth stressing that 12 to 18 months would be fairly fast. It’s almost unprecedentedly fast by typical vaccine timelines. So the question is why does it usually take so long, perhaps? And maybe one way of looking at it is to go through the stages one might do to develop a vaccine and manufacture it. And maybe that would give some insight as to why this might take awhile.
So the initial step is sort of doing basic science or preclinical work in animals or cell culture. Basically to see if your vaccine does what it’s supposed to do, which is essentially provoke the right immune response. And then once you’ve got something which seems to work in your animal or whatever, you then want to see if it actually is safe to give to a person. And so this is usually what’s called phase one study, which is a phase of study where you give small groups of people vaccinations to test safety. And particularly with coronavirus vaccination, that is a major worry insofar as what we saw in previous attempts to vaccinate against something like SARS was these vaccines could backfire, in that they can actually enhance disease rather than protect against it through a variety of mechanisms, which obviously is very bad. You don’t want to mass administer something that then actually makes people have worse outcomes rather than protecting from it. So that isn’t straightforward to navigate.
And then once you do that, you can then run what’s called phase two and phase three trials, where you basically try to test efficacy. Does it actually protect you from the infection? Trials can take quite a while, because you have to maybe follow up for quite a long time to see how much protective effect you’re really getting. I think there was a recent proposal by Lipsitch, Eyal, Smith: which is you might be able to say sometime if instead of doing the typical way we do it, which I described just now, you do what’s called a challenge study, which is sort of what you do, as it were, safety and efficacy studies at once on a population.
So, this essentially means you give someone a vaccine, and then you give them the agent which causes the infection on a sort of RCT basis and see if it actually does work. Obviously, the ethics issues around that are very fraught, which they cover in their paper, which might be worth having a link. But maybe something worth contemplating in terms of maybe saving you some time. And we do see vaccine challenge studies done in some contexts. I know there’s one for malaria. There’s been other ones as well.
What can you do personally?
So typical recommendations to give everyone would very much be good citizenship norms of what typical governments are also recommending people do. And so these are maybe not in good order at the moment but it’s like, “Wash your hands regularly before having food, before going out, before coming back. Generally, if in doubt, wash your hands”. There’s a 20 second recommendation. There’s also a six stage hand washing technique you can look up if you really like. There’s also the respiratory hygiene issue of “Please don’t cough into your hands but cough into a tissue or, if worst comes to worst, inside your elbow or something”.
When it used to be relevant there was obviously “Please isolate yourself if you think you might be unwell, and don’t come into work when you’re sick”. Obviously now in many countries, including my own, the key recommendation is essentially this, which is to avoid all nonessential travel and avoid all nonessential contact with others. And the more people who do this, I’ll expect the better things will be. So I struggle to emphasize it enough in terms of doing all of those things. Now, in terms of particular ways to help, I know 80K published,… Well a couple of days from me saying this, a post on if you’re mired to help, what you can do. I don’t have many obvious additions to this list. In terms of the question of whether rather than what, I would maybe strike some note of caution for a few reasons.
One is that this is probably now maybe the least neglected topic on the planet at the moment, and so the window for having a really outsized impact, like being early, is closed. And this reason may be the case that folks that have prior knowledge or expertise in certain areas, there may not be very good things that they can do to contribute versus what they will be doing otherwise. Because there are still many other problems in the world unfortunately besides COVID-19, and those problems haven’t gone away. And so whether to switch from one to the other is uncertain. It’s also something I’m somewhat grappling with myself as I discussed earlier. So maybe, but maybe not and maybe less so if you don’t have a relevant background which would make you well positioned to contribute would be my best guess.
Global catastrophic biological risks
By any commonsense definition of the term COVID-19 is a global catastrophe, but what we tend to have in mind when we talk about these things are events of such large magnitude that they place the long-term trajectory of humankind in peril. There are a few different definitions of what GCRs are. That’s one. Open Phil’s one talks about how it could globally destabilize enough to permanently worsen humanity’s future or lead to human extinction and you get things along these lines. So it’d have to be like extremely, extremely bad events. And so I don’t think any pandemic in human history has ever really got to that sort of level.
So things like the Black Death, or 1918 influenza or things like the Justinian plague I also don’t think other major current health crises at the moment would also count as these sorts of risks. So, for example, I don’t think antimicrobial resistance is a GCBR, nor HIV/AIDS and so on and so on and so forth. None of which is meant to say these things are trivial or they aren’t important or anything along those lines. But it’s to sort of give a sense of what I have in mind, is events of a greatly different order to these undoubtedly extremely severe threats to global health. And so given COVID-19 falls in this set of very severe threats, it nonetheless doesn’t rise to the level of a threat to human civilization, which I guess you can consider reassuring, although it’s obviously not much for reassurance.
Accidental vs. deliberate misuse of biotechnology
We haven’t really seen many events which have been human caused which are similarly bad to naturally arising events like the typical death toll from scientific accidents or by terrorist attacks or anything else. It’s comfortably less than most other infectious diseases at any given year. So you’re often trying to weigh up within this, which seems risky given the lack of a track record.
And there’s also, I guess, another annoying philosopher’s point whereby the distinction between accidental and deliberate isn’t perfectly crisp. So you can imagine a Dr. Strangelove scenario where someone deliberately makes something very nasty but then another agent uses it without authorization: so it’s the unauthorized use of something that’s deliberately made, but that’s somewhat an accident by light of the person who made it in the first place. Or there could be a thing whereby someone makes something very nasty and accidentally deploys that without intending to. Which again there’s this mix between… Well, you’re deliberately making something very bad, but you weren’t deliberately like releasing it to cause harm. So that’s like a small point. But in terms of the general sketch. One expectation, well hopefully one expectation is, there are more people who are well-intentioned than badly intentioned, so maybe there’s a higher rate of people who have good intentions who then make mistakes versus people with bad intentions doing these deliberately.
That being said, if you’re trying to cause a very, very bad thing to happen, you’re probably more likely to achieve it. Trying to do it deliberately rather than doing so by accident. But all of this is deeply uncertain. The evidence I’ll offer in favor is conjecture: is if you look at other things in terms of single event casualty counts. Maybe one comparison would be, for example, motor vehicle accidents. So most of those happen by accident, and there are far more accidental deaths from cars, roughly speaking, than people deliberately using cars kill each other. But if you look at something like the largest casualty events involving a car or indeed a plane or other things, you see that most of these are from deliberate acts of misuse. So unfortunately, vehicle ramming attacks, for example, tend to have a much higher average death toll than the typical car accident, even though there’s many more car accidents.
Articles, books, and other media discussed in the show
80,000 Hours Annual Review – December 2019
80,000 Hours work on COVID-19
- Landing page with all our COVID-related research and links to the top resources we’ve found
Good news about COVID-19 (our most viral article in a few years)
COVID-19 essential facts and figures
How to best overcome COVID-19 through work and volunteering
Top donation options
List of 200 specific job vacancies, volunteering opportunities & funding sources
The 12 best policy steps to stop pandemics including this one (podcast)
Introduction to Greg’s problem profile on reducing catastrophic biological risks more generally
Greg’s work
- Reducing global catastrophic biological risks
- Greg’s personal site
- In defence of epistemic modesty
- Reality is often underpowered
- Information Hazards in Biotechnology by Gregory Lewis, Piers Millett, Anders Sandberg, Andrew Snyder-Beattie, & Gigi Gronvall (2019)
Everything else
- How does the offense-defense balance scale? by Ben Garfinkel & Allan Dafoe (2019)
- How can doctors do the most good? An interview with Dr Gregory Lewis by Pablo Stafforini (2015)
- Living High and Letting Die: Our Illusion of Innocence by Peter Unger (1996)
- Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand by Neil M. Ferguson et al. (2020)
- The Black Death on Wikipedia
- The Plague of Justinian on Wikipedia
- The Spanish Flu on Wikipedia
- The Columbian Exchange on Wikipedia
- The Justianic Plague: An Inconsequential Pandemic? by Lee Mordechai, Merle Eisenberg, Timothy P. Newfield, Adam Izdebski, Janet E. Kay, & Hendrik Poinar (2019)
- Event 201: A Global Pandemic Exercise — The Johns Hopkins Center for Health Security
- The next outbreak? We’re not ready — TED Talk by Bill Gates
- Human challenge studies to accelerate coronavirus vaccine licensure by Nir Eyal, Marc Lipsitch, & Peter G Smith (2020)
- Manufacturing medical countermeasures against catastrophic biothreats
— Daniel Gastfriend (EAG: SF 2019) - Policy Brief: Evidence-Informed Social Distancing Policies for African Countries by IDInsight (2020)
- Nextstrain
- Drew Endy Lab
- Barriers to Bioweapons: The Challenges of Expertise and Organization for Weapons Development by Sonia Ben Ouagrham-Gormley (2014)
- Ways people trying to do good accidentally make things worse, and how to avoid them by Robert Wiblin and Howie Lempel (2018)
- Scientific Advisory Group for Emergencies (SAGE): Coronavirus (COVID-19) response
- Maximal Cluelessness by Andreas Mogensen (2019)
- The Moral Value of Information by Amanda Askell
- Doing Good Better: How Effective Altruism Can Help You Make A Difference by William MacAskill (2015)
- The Precipice: Existential Risk and the Future of Humanity by Toby Ord (2020)
- IMDB: Dr Strangelove (1964)
Transcript
Table of Contents
- 1 Rob’s intro [00:00:00]
- 2 The interview begins [00:03:15]
- 3 What is COVID-19? [00:16:05]
- 4 If you end up infected, how severe is it likely to be? [00:19:21]
- 5 How does COVID-19 compare to other diseases? [00:25:42]
- 6 Common confusions around COVID-19 [00:32:02]
- 7 What types of interventions were available to policymakers? [00:46:20]
- 8 Nonpharmaceutical Interventions [01:04:18]
- 9 What can you do personally? [01:18:25]
- 10 Reflections on the first few months of the pandemic [01:23:46]
- 11 Global catastrophic biological risks (GCBRs) [01:26:17]
- 12 Counterarguments to working on GCBRs [01:45:56]
- 13 How do GCBRs compare to other problems? [01:49:05]
- 14 Careers [01:59:50]
- 15 The response of the effective altruism community to COVID-19 [02:11:42]
- 16 The response of 80,000 Hours to COVID-19 [02:28:12]
- 17 Rob’s outro [02:36:22]
Rob’s intro [00:00:00]
Robert Wiblin: Hi listeners, this is the 80,000 Hours Podcast, where each week we have an unusually in-depth conversation about one of the world’s most pressing problems and how you can use your career to solve it. I’m Rob Wiblin, Director of Research at 80,000 Hours.
Today, we’re taking a step back towards non-COVID-19 content — with an episode that spends just two-thirds of its time dealing with COVID-19.
Like many others, we’ve been focused almost exclusively on the global pandemic for the last few weeks, but the last third of today’s interview is a reminder that some of the other most pressing problems in the world haven’t gone away.
Dr Greg Lewis worked as a doctor before moving to Oxford’s Future of Humanity Institute to research potential catastrophic risks from advancing biotechnology — basically, biological threats that really would make COVID-19 look like the common cold.
Greg wrote our lovely new problem profile on ‘Reducing global catastrophic biological risks’. We’ll link to that in the show notes and Keiran made an audio version which should be the previous entry in this podcast feed.
And today Greg’s speaking with my colleague Howie Lempel, who’ll be familiar to regular listeners.
He was a guest far back in episode #4 Howie Lempel on why we aren’t worried enough about the next pandemic—and specifically what we can do to stop it, and then joined the 80,000 Hours team in 2018.
He was also my co-host back on episode number 73 – ‘Phil Trammell on patient philanthropy and waiting to do good’, which aired all the way back on March 17th, 2020 – which now seems like an aeon ago.
We’ve also done two COVID-19 themed episodes together, the latest is called ‘Rob & Howie on the menace of COVID-19, and what both governments & individuals might do to help’ and came out on March 19.
But today is Howie’s first episode hosting by himself. The team thought he did a great job, and we’re excited for him to host more episodes in the future.
If you do want to read more about COVID-19, the 80,000 Hours team has worked overtime lately to produce a fantastic package of 10 pieces about how to stop the pandemic.
That includes an article on how to use your talents to solve the crisis, one on where to direct donations, a database of 250 job opportunities and 60 funding sources, a guide to the essential facts about the disease, and if you need a pick-me-up to keep going, a piece on some of the good news we’ve seen in March.
It’s really fairly comprehensive.
Please take a look and share any you think will help people you know make a difference. You can find those at 80000hours.org/covid-19/.
We also just released our annual review for 2019, in case you want to use any extra time you’ve got on your hands on getting to know exactly what we do at 80,000 Hours. We’ll also stick up a link to that, and all of our COVID-19 content, in the show notes.
Alright, without further ado, here’s my colleague Howie Lempel interviewing Greg Lewis.
The interview begins [00:03:15]
Howie Lempel: Today, I’m speaking with Greg Lewis. Greg researches potential catastrophic risks from advancing biotechnology as Acting Head of the Biosecurity Research Group at Oxford’s Future of Humanity Institute. While there, he’s also a DPhil student. He has a medical degree and a master’s in public health from Cambridge, and has worked as a junior doctor and a clinical fellow in public health medicine. Within the effective altruism community, a lot of people know Greg for being an early promoter of earning to give, and for his advocacy on behalf of epistemic modesty. He also recently wrote a problem profile for 80K on global catastrophic biological risks. Welcome, Greg.
Greg Lewis: Thank you. Thank you for having me, Howie.
Howie Lempel: And where are you joining us from today?
Greg Lewis: So I’m enjoying the great indoors in Oxford, which is what I’ve been doing for the last couple of weeks. So far so good. I’m a researcher, so not too much has changed – just the desk I’m sitting at.
Howie Lempel: Fantastic. Yeah. I have recently come out of personal isolation which changes my life essentially not at all. And I am still staying in place in my apartment in London. And so that means that Greg and I are doing this recording remotely. There’s a chance that the audio quality will not be at our usual standards, so I apologize for that. So I guess, just to get things launched off, what are you up to at the moment, Greg? And why do you think it’s important work?
Greg Lewis: Yeah, so I try and do a few things. I mean, principally I’m trying to do a PhD in mathematical biology here at Oxford. But I also get some extracurricular activities as well. One of which is, as you note, I do work at FHI on global catastrophic biological risks, and this comprises maybe a few different things. One is more overarching strategy work, trying to get a better understanding of the risk landscape and which measures have the greatest promise of mitigating these risks. Another is maybe more directly relevant, or maybe shovel-ready things one can do to contribute. This is maybe particularly on my mind given the events around COVID-19. I also try, where I can, to help the emerging community of people in effective altruism and also outside it, who share my concern about global catastrophic risk and are looking to contribute. So that’s a rough survey of what I try to get up to.
Howie Lempel: Great. And can you maybe give an example of what a project might look like in each of those areas?
Greg Lewis: Sure. So at the moment, for my PhD, I’m, in a sense, trying to get a fairly abstract but hopefully worthwhile understanding of the immune system and when it proves to be beneficial and when it doesn’t from an evolutionary perspective, which might give some broader insight into the challenges I try and work on across FHI. For broader strategic understanding, it’s looking at various concepts which are often borrowed from other fields to see if they can be usefully deployed to GCBRs.
Greg Lewis: So one is, which I know my colleagues Allan Dafoe and Ben Garfinkel have done are things called “offense-defense balance”, the idea which is if there’s a conflict between an attacker and a defender, when is this conflict favoring one side or the other in terms of structural factor which might favor one versus the other? And then how does that change perhaps as certain things scale up, which may have some relevance in terms of if the landscape around potential misuse of biotechnology changes, what things were you concerned about? What things can we push on which gives the good guys a robust advantage over the bad guys?
Greg Lewis: With respect to the EA community, I occasionally get referred to people who are early on in their career, who are interested in this area and working out what next steps to take. I also have, as you say, recently wrote a problem profile on this broad area, hopefully to inform people of what this problem looks like, and where they can contribute, and how to weigh it up versus all the other problems in the world. And with respect to any sort of direct projects, there’s like bits and pieces in-house.
Greg Lewis: At the moment, one thing I’ve been looking at is genetic engineering attribution, which is essentially trying to infer from the engineered genetic sequence who was its likely author, which has some potential security benefits if that can be done. I’m working out the policy around that. I’m also trying to think of ways if I can contribute usefully to COVID-19. But it’s a little bit early to say for most of those things how useful or important they will turn out. I guess in some strange sense I’m sort of hoping my work doesn’t prove very important, because the problem I worry about isn’t really a problem after all. I guess we shall see.
Howie Lempel: Yeah. So that’s like a pretty wide range of work. Do you have thoughts on how you came to those priorities or how you prioritize among them?
Greg Lewis: Yeah, so I can give my origin story which is how I got into the broad area; I have a much crisper picture of this than how I prioritize between these things. My hunch is that I’m probably spreading myself too thin, it would be nice to have a sense of stronger focus but that’s, unfortunately as I’m finding, somewhat easier said than done. But with respect to the general point, I worked as a doctor for a bit. Whilst I was in medical school, I was wondering how much good to do.
Greg Lewis: I sort of got into EA via folks like Will MacAskill and a guy called Peter Unger who wrote a book called “Living High and Letting Die”. And I began to apply this mindset to clinical practice to work out, in a sense, how much good does a doctor do? The answer to that was not the most promising. So I thought, “Well, what can I do related to, or instead of medicine, which will have a higher impact?” And I thought public health might be a potentially good option, so I sort of moved into that around the same sort of time, which was around 2012, which is a while back.
Greg Lewis: I was also beginning to be exposed to or interested in longtermism. I also wondered whether there could be a danger; could there be biological threats to this long-term future as well as those which were widely discussed at the time on things like AI? And so that’s sort of how I got into this area. I ended up moving to FHI a couple of years ago, and that’s how I got to where I am now.
Howie Lempel: All right. And so I guess that was the path to arriving at FHI. And so one question is just like, it’s a really big career change. I think most doctors are just not looking to radically transform fields. Do you have a sense of what it was that made you open to making the big switch? Or what felt like it was driving the decision?
Greg Lewis: I’m not entirely sure. I mean, the story I would like to tell about myself would be something like, “Oh, because I’m just so good at trying to do the right thing, I just obviously looked at the considerations and just followed the balance of reason wherever it led me”. I hope that’s mostly true. So I hope I was principally motivated by my judgments on which things seem more or less promising in terms of having a greater or lesser impact. And certainly there are other parts to that, but I don’t have very good insight into what those are. I mean a common suggestion which people have made is I didn’t actually enjoy clinical practice very much, so I was eager for an excuse to jump ship. I don’t think that’s true actually. I actually still miss the patients even now. So I think that’s part of the story.
Greg Lewis: There may be other parts which are somewhat less edifying, which sadly I genuinely don’t know myself, although I suspect they’re there.
Howie Lempel: Did it feel like a hard decision?
Greg Lewis: No, actually. So there are a few things which I miss of what I was doing before. I do miss patient care. But on balance, I do quite enjoy it. There are some personal downsides to working as a clinical practitioner; your nights and weekends are seldom your own. Obviously the work can be quite long hours. It can be quite stressful in various senses. And so from a personal perspective, there are upsides and downsides. But hopefully from, I guess the point of view of the universe if you excuse the term, it’s hopefully much better to be doing the work I’m doing now than the work I was doing as a junior doctor working on a ward for example. So I don’t have many regrets about how I’ve turned out.
Howie Lempel: If you’re up for sharing, are there personal upsides or personal downsides from your current work that you feel are particularly salient or acute for you?
Greg Lewis: Nothing really beyond that. I think I mentioned all the major ones. I mean, the principal upside is just the avoidance of medicine’s taxing, long hours. All the things that you usually talk about in terms of why being a doctor is hard were true to varying degrees in my own experience as well. And so insofar as I’m not doing that anymore, I guess those are, in some sense, upsides. But as I mentioned, on the downside, I did genuinely enjoy it when I was working as a doctor.
Greg Lewis: And perhaps wrongly, but nonetheless did feel sort of like you’re being a little bit of a hero on the wards like, as it were, healing the sick. And I think most doctors grow out of that story after a while, but I think I was still in my fairly naive phase at the time I was leaving it. And so there’s still some like nostalgia around that. But those are the main ones. But as I say, on balance I don’t have any great personal regrets. I think it’s like, on balance, it would’ve been good for my personal life, and, as I said, hopefully good for the wider world as well.
Howie Lempel: Great. It seems like it often works out that way. People, if they feel like they’re doing things that are good for the wider world, you know, often that turns out for them personally too.
Howie Lempel: Yeah. So when you talk about this bit of nostalgia around being a doctor. I know I have some EA friends who are former doctors who have felt a bit of a pull to take a sabbatical from where they’re currently working. And they get into a hospital and start doing COVID responses. Is this a thing that you have either taken seriously, or even just some part of you feels?
Greg Lewis: No, it’s definitely crossed my mind. Especially because I think… Because I left practice a few years ago, the NHS or the GMC, which is the General Medical Council of the UK, has recently re-registered doctors like myself. So I now, in theory, could practice medicine and go again. So I might get various hospitals ask me to, as it were, return to duty. Which obviously, there’s a mix of considerations with respect to that, both personally and more generally about whether that’s a great idea or not.
Greg Lewis: I mean a couple which spring to mind: I last actually touched patient anger, as it were, five years ago. And unfortunately a lot of skills in medicine are pretty perishable. So I’d worry that I’m very severely out of practice, and there’s actually good research on this which I looked up, suggesting that after two years it’s actually quite a lot of effort to get back to where you were. So that’d be like one motivation. There’s also the thing of that given my background has now more moved towards public health and policy and things like that, whether if I was going to spend all my energy responding to COVID-19, whether I’d be best placed as probably a reasonably bad frontline doctor at least at first, versus maybe a somewhat better person working on more like the policy side or similar. But in honesty, I don’t actually have a very crisp idea of how I’m going to address this dilemma, but it is definitely weighing on my mind.
Howie Lempel: Yeah. So COVID-19 is one of the two topics that I wanted to chat with you about. Mostly because Rob and I have rushed out a couple of podcast episodes on the topic recently, and we are both very self aware of not being experts, and so bringing on someone with some background as a doctor and in public health, and at least in adjacent fields, to ask them questions and to show us where we’re wrong seemed really valuable. And then later on, we’re hoping to talk about the global catastrophic biological risk profile that you’ve written up, and the sort of case that you’ve made for working in that area. Does that general organization sound okay to you?
Greg Lewis: Sounds good. I feel almost obliged to say I would hesitate to call myself an expert on probably any of these areas. I mean, to be an expert on COVID-19, generally you’d have to spend like a century of background in all the various areas, which I definitely haven’t done. And there’s actually quite a lot of data which keeps coming out that I fear that by the time this podcast comes to air, it may already be out of date. But I will nonetheless try my best. And GCBRs have this similar property of being fairly pan-disciplinary and also very complicated. So I can do my best, but I wouldn’t want to offer a great guarantee of quality. But I guess it’s for the listeners to decide.
Howie Lempel: A helpful disclaimer. Yeah. So I guess, just give some context, what has your relationship with the outbreak been so far? How closely have you been following it?
Greg Lewis: So I followed it fairly closely. It’s obviously a matter of interest to probably most people on the planet by now. But insofar as I used to work in public health and things related to that, there’s obviously a particular professional interest to try and, as best one can, keep abreast of the relevant things. I also, sort of in the early days, was sort of helping out FHI in working out how the office should best respond to this as well, which provides a further motivation to try and keep track of things. So yeah, maybe like a reasonably well-informed layperson overview I might be able to provide.
What is COVID-19? [00:16:05]
Howie Lempel: Cool. And yes, we’re going to ask Greg to give that kind of overview. For listeners who’ve already had that, totally encourage you to skip ahead. But yeah, so just to give a sense of what is this disease? Where did it come from? How scared should we be of it? I was wondering if you could just catch us up. So maybe to start with, you know, when did this start? Where did it come from? What type of a disease is this?
Greg Lewis: Sure, I’ll try. I should stress that a lot of this area is shrouded in quite a lot of uncertainty. But anyway, COVID-19 is this new infectious disease in humans. It’s caused by a coronavirus, which is SARS-CoV-2. We think this emerged probably somewhere in or near Wuhan, China in late 2019. We think it’s something called a zoonotic disease, which means the virus used to, as it were, infected other species, and then started infecting humans. But exactly which species it originally infected and how it came to start infecting humans is very uncertain. There’s lots of conjectures in the literature, but I don’t think anyone really knows for sure.
Howie Lempel: Do you know how we are so confident that it’s zoonotic?
Greg Lewis: Well some of the evidence that people have been looking at are comparing the genetic sequence of a virus to the genetic sequence of other viruses. And you find quite close matches between this virus and another coronavirus which would infect bats, and I think also pangolins, although I think the relative similarity is controversial. So that’s perhaps one of the main lines of evidence which leads one to suspect that this virus was originally in another species and crossed over to people.
Greg Lewis: It’s also worth noting that this so-called zoonotic transfer, or zoonotic virus effect, in which one species is going on to infect another species, is fairly commonly observed and hypothesized for other emerging infectious diseases. We think this had like a large part of the story to do with things like the Ebola virus, maybe HIV, various pandemic flu strains we think involve recombination in another species and then end up jumping back over into humans. So given that the mechanism isn’t so implausible, and you find these suggestive things when you look at the genome, all of this adds up to be suggestive.
Howie Lempel: Got it. That’s really helpful. Okay, great. So we’ve talked a bit about where the virus started from. Can you talk a little bit about how it’s spread from there?
Greg Lewis: Yes. So obviously this is contagious. We believe that principally it’s spread through respiratory droplets, either directly. So an infected person coughs, and the droplets which are in the air for a little while may be inhaled by those close by. Or indirectly, so someone coughs into their hand, they touch an object, another person who’s not infected touches that object and then touches their face so transferring the virus to them. There have been various other conjectures of possible sources of spread. There’s some suggestion that, on occasion, a virus can be spread by aerosol, although that seems to be like a minority.
Greg Lewis: There’s somewhat a continuum between droplet spread and aerosol spread anyway. There’s also some conjecture that the virus could be possibly shed in feces or stool. So there’s a possibility of fecal-oral transmission. But these are mostly conjectures or cannot be ruled out sort of things, rather than the principle mode of spread which definitely seems to be this respiratory droplet sort of route.
If you end up infected, how severe is it likely to be? [00:19:21]
Howie Lempel: So we’ve talked a little bit about how the disease is spread. If you do end up infected with the disease, how severe is it likely to be?
Greg Lewis: Sure. So assessing severity is quite complicated. One of the key challenges is that for many people COVID-19 seems to give either no illness whatsoever, so no symptoms or very few symptoms, or a reasonably mild disease. Which means you sort of have this iceberg effect whereby the people you see in hospital are sort of the tip of it who are the most severely unwell, and it’s hard to work out from it how many people have also been infected but haven’t had such severity.
Greg Lewis: Maybe like the most widely used data is from a very large, I think 70,000 person study in Wuhan. So we think there’s some fraction who may be asymptomatic. Of those who end up getting recognized as a case, we think about 80% of those are, relatively speaking, mildly unwell with something similar to a flu-like illness with a fever, tiredness, or a dry cough. Of the remaining 20%, 15% are more seriously unwell and require hospital care of varying types. And 5% are critically unwell, and so might require things like mechanical ventilation or other signs that they are very severely sick.
Greg Lewis: The so-called case fatality rate is what portion of these people die. And for that, you get figures from, I think, 1% to 3% if you estimate based on the cases you see. The challenge of that is that isn’t quite the same thing as the infection fatality rate, which is possibly the question you’re more interested in. And so conditioned on me being infected, how likely am I to die, is sort of the question we care about more than if I’m infected and I’m recognized as a case, how likely am I to die?
Greg Lewis: And to try and adjust this, it’s quite tricky. On the one hand, all those people who are currently known to be cases, you don’t know how all of them will turn out, so you can’t necessarily just assume that everyone will recover and survive. Well obviously you definitely hope they do. And, on the other hand, given this iceberg effect for these subclinically ill asymptomatic people, you also don’t know what the denomination really should be. And there’s been various attempts to adjust this based on various sources of data, and probably the best source, or the best source I rely on, is an Imperial study. One of like the 12 reports they’ve done so far, which estimates the infection fatality rate of 0.9% with quite a lot of uncertainty.
Greg Lewis: It’s also worth addressing that this risk isn’t uniform across a population. So the risk of death is much lower if you’re young and healthy. To my understanding there’s been no one who’s died from this disease under the age of 10, and I certainly hope that’s true and continues to be true [Alas no longer true, given some case reports – Ed.]. But by contrast, the infection fatality rate they estimate for people who are over 80 years old is around 9%. So that’s obviously 10 times higher than the rate across the population. We also think that preexisting conditions of various sorts would also increase one’s risk as well, both probably of getting more severely unwell and also unfortunately of dying too.
Howie Lempel: Okay. So it seems like you’re taking a lot of your intuitions on this from this Imperial report that estimates an infection fatality rate of around 0.9%. As you said, these vary across contexts. Do you know what context that was attempting to model?
Greg Lewis: Yes. I think this was, to my recollection, modeling as it were a status quo scenario. So maybe it’s easier to stress what this may be sensitive to. So one area which it maybe proves to be higher or lower, is it depends on, in a sense, how good can you treat people who get unwell? And so, for example, if we get new developments in how to better treat people who become sick with this, then you’d expect the IFR to go down. Contrariwise, which is a major worry confronting a lot of policymakers right now, is if your hospital services become overburdened. So if there’s a lot of people who are very unwell at the same time and you have limited capacity and you can’t treat all of them, this will probably contribute to excess mortality.
Greg Lewis: Another concern is that may not just apply to people who are sick with COVID-19, but also people who get sick for other reasons during the same period. So people with heart attacks or strokes or other serious medical conditions. If they’re having to seek care in an environment where already hospital services are greatly overburdened, you’d expect unfortunately them to receive less good care and a worse outcome as a result of that.
Howie Lempel: Got it. Good point. And then I guess one thing that I’ve noticed in these types of discussions of severity is that it’s really easy to get anchored on the fatality rate numbers. And so I’m wondering… I guess number one, whether you know anything about morbidity from COVID. Like how much of an effect we think that ought to have. But also, we hear about these enormous numbers of people who maybe might not end up in an ICU, but who end up spending a bunch of time in a hospital bed. Do you have any sense of what’s going on with those folks?
Greg Lewis: Maybe. I mean, so with respect to morbidity, COVID seems to present as like an acute illness which then people recover from. Obviously a concern has been raised on, could there be chronic long term effects? So even though you recover from the infection, are that some consequences for your health after you’ve recovered? And that’s unfortunately very hard to know for sure because no one’s been followed up for this disease for more than three months. There are like a variety of factors you can speculate upon, which could maybe increase or decrease your estimates. So obviously there’s been some observation of chronic health effects of people who were infected with SARS, which is somewhat related. In contrast though, other coronaviruses, like the common cold, don’t really have very significant long run effects. And then there’s other things you can deduce from, like, for example, if it was an acute infection, which seems to get cleared so people have negative PCRs. Sort of it’s suggesting they’ve got rid of most of the virus, is not what you’d typically expect for a virus which causes an infection and then causes chronic consequences thereafter. Although unfortunately, as I’m maybe indicating, nothing can crisply be ruled in or ruled out. There’s also potentially an effect where both you become very severely unwell, it may take you longer to recover, and maybe there will be some long term consequences of that as well. But all of this is unfortunately no better than conjecture either way. We’ll find out more as time goes on.
Howie Lempel: Got it. Makes a lot of sense.
How does COVID-19 compare to other diseases? [00:25:42]
Howie Lempel: So you’ve done a good job characterizing the basic situation and sort of lining up what this virus looks like, and I think it’d be helpful to contextualize it a bit. So you can think of, like on the one hand, you hear comparisons between COVID and the seasonal flu often from people who are least concerned. And then on the other hand, you might say like, “Look, this is the biggest pandemic that the world has faced in a while,” and kind of go pretty far on the other side and start to worry like, “Is this going to be like a serious global catastrophe?” And I’m curious, especially because you study those incidents sort of all the way on the end of that curve, like how you think about where COVID fits in?
Greg Lewis: Sure. So I think it has been very unfortunate that people have suggested it’s similar to seasonal influenza. Although seasonal influenza does share some features with COVID-19, it’s much less severe in terms of how many people it makes severely unwell. How many people end up dying from it, and so on and so forth. So it’s definitely substantially worse than, as it were, the typical flu season. In terms of how to rank it out on the tail of very bad events, people making comparisons of, say, the worst pandemic since 1918 is sadly, I don’t think, hyperbolic.
Greg Lewis: It’s still hard to compare pandemics to each other because the data we get from this one is firstly very uncertain and we’re not entirely sure, for example, how well will the measures to address it or contain it work, and it’s also actually very hard to figure out historically how bad some pandemics were, on which I suspect more later. But it seems, at the moment my best guess would be that this seems to be worse than other influenza pandemics we’ve seen over the course of the 20th century, with the exception of 1918. And so it seems like the worst since then is unfortunately a reasonable guess.
Greg Lewis: In terms of, as it were, does this count as a global catastrophic biological risk? Then in the colloquial use of these terms it definitely does. So it’s definitely a global catastrophe which is biological. The only one which doesn’t really apply is risk, because it’s already happening. It’s not really a risk anymore, unfortunately. But typically, and again, maybe more later, the way this term is used in the literature is sort of events which are so bad that they pose a credible threat to human civilization as a whole, roughly speaking. I don’t think really any historical pandemic has really posed such a grave risk, notwithstanding that they are humongous and outrageous humanitarian catastrophes. And thinking back to something like the Black Death or the 1918 flu, COVID-19, which I don’t think will become as severe as either of those two things, I don’t think it’s like a GCBR either in that sense.
Howie Lempel: Got it. So yeah, I think it would be interesting to talk through some of those historical pandemics just to get a sense of what could happen without rising to the level of it being a GCBR. But maybe like another way to just sort of get calibrated on like how big of a deal this is. People have been talking about how we haven’t seen anything like this since the Spanish flu. This is like a once-in-a-century event. Does that seem accurate to you? And how surprised were you that something like this happened? Is this like a big update for you on how bad pandemics can get, or how frequently they arise?
Greg Lewis: Sure. So I think calling it sort of like ‘worst since 1918’ is reasonable. I mean it’s hard to say. Maybe as one hopes, we’ll see this great reduction in the current exponentially increasing trend of infections and deaths, such that it turns out to be much less bad than something like the 1918 flu. But unfortunately it’s still too early to say. In terms of, was I surprised by this? I definitely don’t want to claim I’m some sort of Nostradamus who predicted to the day or the hour that there would be a major pandemic which would cause a grave humanitarian catastrophe. Unfortunately, I do think that a lot of people working in the areas like public health, pandemic preparedness, epidemiology, have been stressing for a very long time that we remain very vulnerable to a pandemic, to emerging zoonotic diseases. Various things we’re doing probably increase the risk of these diseases arising. And we have very limited means of, if it does happen, to respond to it in a way which would like dramatically reduce the suffering and death it would cause.
Greg Lewis: And so I think, in that sense, it’s maybe somewhat depressing that this wasn’t exactly like a bolt of lightning from a clear sky. People were saying there were clouds on the horizon for years and years and years. I mean, CHS had a tabletop exercise discussing how an emerging pandemic could cause lots of problems, and these problems we’re unfortunately basically experiencing now. I mean Bill Gates had a TED Talk a while ago saying we’re not ready for the next pandemic, and unfortunately it seems like he was right. And you know, if you look at most people who’ve been writing on global health security for quite a long time, they’ve kept stressing, “This is a serious risk. We’re not sure when, but it’s probably a matter of when rather than if. And if it does happen, we’re going to be a lot of trouble”.
Greg Lewis: And so in that sense, unfortunately, this wasn’t a great surprise, and for that reason it’s not been a ginormous update for me, because I already thought it was going to be a pretty big danger, and the danger happening doesn’t really do much to change that. Another challenge here actually, which may also come up later in the program, is these events are rare and so getting like a very good sense of the evidence of a single event is very hard. Reality, I guess, is somewhat underpowered to assess whether, let’s say, the rate of pandemics is increasing or decreasing over time, especially given all the challenges in trying to assess all the evidence, and we don’t observe things very well.
Howie Lempel: Yeah, cool. So I guess the takeaway is this is a pandemic serious enough to be a candidate for a once-in-a century-event, even if things are still early. And we certainly have some hope that things will end up looking better than we expect, and also that the public health pandemic preparedness community, while they’re not fortune tellers, they have been concerned about this kind of thing for a reasonably long time. Does that sound like a fair summary?
Greg Lewis: That seems fair to me, yes.
Common confusions around COVID-19 [00:32:02]
Howie Lempel: Great. So I guess maybe moving on, there are, I guess, specific questions about characteristics of the virus and the disease that seem to come up over and over again, where I haven’t been able to get an answer that I feel like I really understand. So shooting it by a former doctor and seeing how that goes just seemed like a good opportunity. So you are not going to be an expert in all of the things that I bring up, but I wanted to see if you were game to sort of go through some of these?
Greg Lewis: Sure, I’ll try. I’m not actually a former doctor yet. I am still on the medical register, just about. I mean, we’ll see if what I say in the next few minutes may cause that change, but I’ll try my best.
Howie Lempel: Great. Yeah, so one concept that comes up repeatedly is that a lot of our data could be biased, or inaccurate, or not measuring exactly what we want because it’s not picking up cases that are asymptomatic or mild cases. And so if you have cases that range all the way from like, “I feel nothing,” to, “I’m in the hospital,” to like, “I am in critical condition” or “dead”, and then only the people who get hospitalized and actually are becoming clinical cases, you’re going to look like all of the cases are really severe. So it matters a lot to figure out how many mild cases, how many asymptomatic cases are out there. So do you want to talk a little bit about anything else that’s relevant about these categories, and why they matter in outbreak response and epidemiology?
Greg Lewis: Of course, I’ll try my best. So one challenge is it’s sometimes hard to distinguish between asymptomatic and presymptomatic. So someone may test positive for a virus before they do have symptoms. They do eventually go on to develop symptoms. And so trying to work out how many people, as it were, remain asymptomatic with this infection is pretty fraught. There’s various data sources you can use, like repatriation flights, the Diamond Princess which is this cruise ship where a lot of people had an outbreak on where we tested most people – almost everyone. And so there’s various attempts like this, but all of them are challenging, because you want to adjust to lots of things when you’re doing this. But it suggests that some proportion of people we think probably remain asymptomatic. And that may also vary by age. We’re not entirely sure.
Greg Lewis: The other challenge is whether people can spread the disease before they develop symptoms. So, as it were, asymptomatic spread. And unfortunately that seems to be very likely, which does pose a big challenge for containment because if you can isolate people who are sick, that gives a better chance of containing it if you isolate all the people who are sick. If some people who think they’re healthy but are, in fact, infected can spread to someone else, who then does become very sick themselves, that poses a much greater challenge.
Howie Lempel: Yeah, so I guess I’ve just always been curious about why there’s so much variation across viruses. Where for some viruses it seems to be the case that asymptomatic or presymptomatic people are actually doing a bunch of transmission, and then for other viruses it’s not until they start showing symptoms, or even like a couple of days into showing symptoms before they start infecting other people. And I was wondering if there’s any sort of known mechanism for why there’s this variance of why this took place?
Greg Lewis: Yeah, so I mean maybe one way to put it is that depending on the mode of spread, you are releasing, to some degree, respiratory droplets just when you’re talking, as well as when you’re coughing or sneezing. So there’s a plausible story whereby if a virus is replicating away but it’s yet to cause you any symptoms, you may still be spreading it without having symptoms. In terms of why some infectious diseases do this more than others, and to varying degrees, I don’t have a very good answer, I’m afraid.
Howie Lempel: Cool. Does that mean that I should be at all more worried about coming into contact with people who are just speaking distance away from me? And I’m having a conversation with them and they’re not coughing. I feel like the sort of general vibe that I’ve been getting is very centered on like, “Don’t get coughed on”.
Greg Lewis: Yeah. So a lot of the physical distancing recommendations you’re seeing from various governments, including my own in the UK, is essentially trying to act as an insurance against this risk of people spreading it to others without either person realizing they’re at risk. So, in a sense, this idea of like, avoid all non-essential contact with others, doesn’t have a rider of like, “Oh, if both of you feel well it’s fine,” partly for reasons like this. But also people may not always recollect what symptoms they have. If you’re coughing like once or twice a day or something, maybe that’s a sign of a very mild infection for argument’s sake. But you may not notice that, potentially, and think you’re well. And so given all these things, there’s this general urge towards just basically making as little in-person social contact as possible as a way of reducing the spread of the disease.
Greg Lewis: If you knew for sure that only people who were having symptoms could spread it, which may have been the case in SARS, although there’s slightly more of a story there, then maybe this wouldn’t be as necessary over and above a milder principle of, “Please isolate when you’re feeling unwell”. But unfortunately that doesn’t seem to be the case, and hence why we’re seeing what we’re seeing now.
Howie Lempel: So another question on these asymptomatic cases is that I’ve now seen a lot of work trying to use fairly sparse data to figure out what percent of infected people with COVID are asymptomatic. And I feel like when I start trying to use data sets that I don’t really know well, I’m not a doctor, or an expert, or an epidemiologist, or a virologist, It’s sort of easy for me to end up doing crazy stuff. So it’s just interesting to me to have some sense of like, what is normal? Like, would it be really weird if half of all infections for a disease this deadly ended up being asymptomatic? Like how would that compare to stuff like the flu?
Greg Lewis: Sure. So I don’t think it’s wildly crazy and wildly surprising to see a very wide spectrum of severity, from things which kill, to infections which people may not even notice they have. So, for example, we know seasonal flu kills a reasonably large number of people every year, yet we also think that maybe, I mean there’s like a review on this… So like 15% of cases of infections of the flu may be asymptomatic. So you’re spreading the entire range there. And so in light of this, seeing this very large variation of a condition which can also kill but also be asymptomatic, it doesn’t seem wildly surprising. Obviously the relevant proportions in each of these buckets of like mild, severe, critical, fatal, asymptomatic could vary a lot, but that you can get all of them at once doesn’t seem very shocking.
Howie Lempel: And do you have any idea of what leads to this very wide variation among patients who are all infected?
Greg Lewis: Yeah, that question’s probably a little bit above my pay grade, but I’ll give it a stab. So there’s probably a lot of factors which intervene on your prognosis: so how the disease will happen based on the individual. And that could be based on things like the initial infectious dose, which is thought to be particularly one worry, potentially where people who work in healthcare, because they might have much larger doses than typical. There’s also considerations around how fit and healthy the person was initially. It’s fairly common in medicine that an infectious disease which causes typically mild illness in one group causes much more severe illness in another for all sorts of reasons related to the patient’s physiology and other things like that.
Greg Lewis: So yeah, as I’m suggesting, it’s like you can noodle around a variety of factors. So in terms of explaining the variance, it’s not necessarily very easy to do, but in terms of that there is such a wide variance, that isn’t so surprising.
Howie Lempel: And then I guess one of the things explaining the variance is age, and you can just see a really large effect there. And I’m wondering if there are theoretical reasons to expect fatality rates to vary by age that much?
Greg Lewis: Sure. So I can offer some stuff I was told in medical school. I’m not sure how much this was expert conjecture versus established fact. But we know that age, for many diseases including infectious ones, tends to be a statistical predictor of outcome. So people who are older tend to have a higher risk of getting more unwell or dying. For a majority of things. In fact, age is often used in various scoring criteria doctors use to try and predict the severity of prognosis from various infectious diseases.
Greg Lewis: Now the reason why that’s the case could be a couple of things. One is that age often correlates with other conditions one might have. So maybe your lungs don’t work as well. Maybe you may have heart disease. You may have some kidney trouble, or other things like this, which may mean that if, in a sense, your body isn’t working as well as it could, but if it faces a further insult or a further challenge, it may respond less well then so it doesn’t have these things. So in a sense, age is being confounded by comorbidities. But there’s also a story whereby it could just contribute even if that’s not true. So my understanding, although I’m definitely not a gerontologist, is that most organ systems, even if they don’t get clinically recognized as one gets older as being worse, are in fact becoming less efficient and less highly performing as time goes on.
Greg Lewis: So for this reason, even if it’s not recognized you have these deficits, as it were, you do, in fact, typically still have them. And in virtue of which, even if you’re aging relatively healthily compared to a younger person, you may still be at higher risk if you have a threat to your health than otherwise. So I guess, in a soundbite, age may only just be a number, but it’s also a number which probably correlates quite well with general physiological functioning, and unfortunately negatively so.
Howie Lempel: Another question that’s come up a lot, especially among current policy debates, is a bunch of questions around immunity. There are questions like, “If someone gets infected, how likely is it that they can get reinfected again, and at what points”? And so, there are some claims out there that are saying things like, “Someone tested negative on a PCR diagnostic machine. Then, a couple of weeks later, they come back, they test positive. Uh-oh. Maybe that means that immunity doesn’t last that long and people can get reinfected”?
Howie Lempel: The reason that this might be really scary is if one of your end goals, potentially, is to achieve herd immunity, where enough people become immune that the disease can’t really continue to spread out that much more, that doesn’t work if everybody loses their immunity. I guess I’m curious about whether you have a take on this; does this pass the initial tests of “This seems plausible. This is a way that lots of viruses work”?
Greg Lewis: Sure. I’m definitely not an immunologist either – there’s many things I’m not, unfortunately. But I can channel those who have looked at this. So, my understanding of what they say is the immunology around COVID-19 is obviously deeply uncertain. That being said, I think most people think in typical cases, I know there’s some exceptions to various other conditions which can be pre-existing as well, but in a typical patient, rapid reinfection seems pretty unlikely. There’s, I think, some animal studies I remember seeing a preprint of which suggested they do maintain, as it were, immunological memory. Once they’re infected, they can get rapidly reinfected again. How long this will last for is obviously deeply uncertain, and so I think people typically would want to offer alternative explanations for these accounts of like, “Oh, they tested negative. Then they tested positive again”. Maybe one of the leading ones being that PCR tests are not perfectly sensitive, and so you give that a false negative result rather than if they truly didn’t have the infection and they picked it up again very shortly thereafter. That’s typically the account people would give, which seems roughly right to me.
Howie Lempel: Right. So another big area of uncertainty for me is I’ve seen some claims that even if you end up sick with COVID and get better, there might be some long-term effects that you’re sort of stuck with for a longer period of time. So chronic fatigue is one that’s mentioned a bunch. Lung damage is another one that’s mentioned. And I have not normally seen these from super rigorous sources that are citing many studies. And so I just don’t know whether or not I should put some weight on these and be worried about this, or treat this as just incredibly unlikely. Do you have an intuition on this?
Greg Lewis: I have a few. I mean, so basically the challenge is, we haven’t followed anyone up for more than three months, which means you can’t really know for sure what any long term effects could or could not be. And so you’re left with trying to adduce from other nearby diseases or other nearby circumstances and try and work out how likely it is. And then you get a very mixed picture. I think with chronic fatigue, we know it comes from people who were infected with SARS, which is somewhat similar to COVID-19, at least genetically. But also, COVID-19 is sometimes like cold viruses which cause common colds, which typically don’t seem to be a major worry in terms of chronic results thereof. It seems reasonably intuitive to me that if you become more severely unwell, that increases the chance both of prolonged recovery, maybe a higher risk of what you might call lasting damage. But again, that is only conjecture.
Greg Lewis: Another thing to say is we might also care about the severity of what the long-term effects actually are. So we’re finding a fair amount about whereby infection with some disease or another may increase one’s risk of something or another later in life, but that may not be something which should hugely keep one awake at night. I mean, if we discover like 20 years hence, COVID-19 infection doubles your risk of a one in a million rare form of cancer, this is a long-term consequence, but may not be a long-term consequence we’re particularly worried about. I mean, for myself, the main thing I’d be worried about if I was infected would be the acute illness, even though that is happily for me a pretty low risk even if I do become infected. That’d be the bulk of my worry, rather than this possibility of, well, I could recover and maybe there’s something down the line which causes me trouble later on. But as I’m hopefully making clear, this is unfortunately all pretty much unknown.
Howie Lempel: Well, it’s good to get that summary and I think I’m going to ask that we move on to start talking about the response to the outbreak.
What types of interventions were available to policymakers? [00:46:20]
Howie Lempel: So I guess once the outbreak started, if you could just talk through what types of interventions were available to policymakers and public health officials?
Greg Lewis: Sure. Maybe I could subdivide into what you might do for an individual patient versus what you might do for an at risk population. So, as unfortunately was noted also quite early on, when you have this new emerging infectious disease, your options for a patient are pretty limited, and your options for populations are similarly so. So, you tend not to have any treatments. You don’t have a vaccine. So, you’re fairly stuck with a variety of essentially non-pharmaceutical interventions. So, for individual patient care at the moment, it essentially remains supportive. This is things like oxygen therapy, mechanical ventilation, other things to try and keep patients as well as possible so that they can eventually recover from the infection and clear it themselves. There are a lot of ongoing trials looking at whether we can repurpose drugs, because they might turn out to be useful in terms of COVID-19, even if they weren’t designed with that in mind.
Greg Lewis: For protecting the population, you don’t have a vaccine and you won’t have one for some time, on which I suspect more later. And so you’re stuck with fairly old fashioned public health measures: things which wouldn’t be particularly surprising to a 19th century public health physician. So things like sanitation, improving hygiene, quarantine and isolation, contact tracing. We are seeing people try and augment things with sort of more 20th, 21st century technological tools. But as I think we’re all observing now, it’s difficult to adequately protect the population from the spread of this disease, whilst also allowing them to continue living their lives as they usually would. It seems like a reasonably hard to navigate trade-off.
Howie Lempel: That sounds right to me and does seem to describe one of the big trade-offs here. So I guess one thing that, in my mind, has really framed thinking about the response is that you sort of have this potential pot of gold all the way at the end of the process where in some amount of time — it seems optimistic to consider maybe 12 to 18 months — you’ve researched, developed, manufactured enough vaccines to make them very widely distributed. And then hopefully the pandemic is over. And I feel like the big question there is just why does it take 12 to 18 months? And it seems like a lot of the other interventions are, in part, trying to buy time to get to that point. So yeah, do you have a sense of what parts of this process mean that we’re waiting many months to like a year and a half, instead of responding much more quickly?
Greg Lewis: Sure. So, it’s worth stressing that 12 to 18 months would be fairly fast. It’s almost unprecedentedly fast by typical vaccine timelines. So the question is why does it usually take so long, perhaps? And maybe one way of looking at it is to go through the stages one might do to develop a vaccine and manufacture it. And maybe that would give some insight as to why this might take a while.
Greg Lewis: So the initial step is sort of doing basic science or preclinical work in animals or cell culture. Basically to see if your vaccine does what it’s supposed to do, which is essentially provoke the right immune response. And then once you’ve got something which seems to work in your animal or whatever, you then want to see if it actually is safe to give to a person. And so this is usually what’s called phase one study, which is a phase of study where you give small groups of people vaccinations to test safety. And particularly with coronavirus vaccination, that is a major worry insofar as what we saw in previous attempts to vaccinate against something like SARS was these vaccines could backfire, in that they can actually enhance disease rather than protect against it through a variety of mechanisms, which obviously is very bad. You don’t want to mass administer something that then actually makes people have worse outcomes rather than protecting from it. So that isn’t straightforward to navigate.
Greg Lewis: And then once you do that, you can then run what’s called phase two and phase three trials, where you basically try to test efficacy. Does it actually protect you from the infection? Trials can take quite a while, because you have to maybe follow up for quite a long time to see how much protective effect you’re really getting. I think there was a recent proposal by Lipsitch, Eyal, Smith: I’m mispronouncing their names, I apologize, which is you might be able to say sometime if instead of doing the typical way we do it, which I described just now, you do what’s called a challenge study, which is sort of what you do, as it were, safety and efficacy studies at once on a population.
Greg Lewis: So, this essentially means you give someone a vaccine, and then you give them the agent which causes the infection on a sort of RCT basis and see if it actually does work. Obviously, the ethics issues around that are very fraught, which they cover in their paper, which might be worth having a link. But maybe something worth contemplating in terms of maybe saving you some time. And we do see vaccine challenge studies done in some contexts. I know there’s one for malaria. There’s been other ones as well. But once you get through all of that, and you’ve actually got a vaccine which is safe and it’s effective, you then have to manufacture and administer the thing. Manufacturing often–
Howie Lempel: Just before we get to the manufacturing, so just for the part that we’ve talked through so far, do you have a guess at how long that part is usually going to take?
Greg Lewis: Many months is my best estimate. So doing a challenge study might save you some time. There’s also the risk, of course, that although you’re doing a lot of candidates currently being tested in parallel, obviously some may not work. Some may fall short at various stages. We often can’t back it for major diseases even now. So, it’s not like you can just guarantee success if you go on a vaccine program, you’ll eventually get one. It might take a very long time. So yeah, it’s quite uncertain as to how long it takes you to even get to a candidate in the first place.
Howie Lempel: Got it.
Greg Lewis: So yeah, with respect to manufacturing and administering. The manufacturing is not straightforward. Daniel Gastfriend gave a good talk on the challenge which comes up with scaling pharmaceutical therapies, like making millions and millions of doses very quickly. And that’s often pretty hard. The only thing we really do this for now is with the seasonal influenza vaccine. And doing it for other things is pretty hard. It’s not always very easy to repurpose things. You need to make one vaccine to make another sort of vaccine, for example. It varies a lot depending on what particular vaccine turns out to be an effective candidate. Some may be easier to scale up than others, but generally, the challenges are quite fraught. Probably rather than giving it much more of a summary, I’ll probably just want to refer listeners to the talk Daniel gave at EAG, which I was also sitting in on, which I think covers it much better than I will now.
Howie Lempel: Cool. That makes sense.
Greg Lewis: And I guess one further thing to say, of course, is that administering vaccines worldwide is not an easy thing to do. Vaccine administration is known to be its own series of fraught challenges. You might need a cold chain, for example, which makes things harder, especially if we’re perhaps going to poorer parts of the world. The time it takes once you have the factory churning out, as it were, all the vaccines, getting it into the hands of people who need it may also take more time as well.
Howie Lempel: Cool. That’s really helpful. Two other things that I’m sure are bad ideas and I’m curious whether you know why they’re bad ideas. So it doesn’t seem like they give people convalescent sera particularly early on. Is there a reason that that’s very risky or just not used all the time?
Greg Lewis: So I’m not hugely acquainted with the literature around this. I know it’s actually being, I think, trialed at the moment for COVID-19. I mean, it requires access to their veins. It’s definitely not so easy as vaccination and also… I don’t think it scales, as well. So, I think it could be done and it could be useful. I’d want to think a lot more carefully before trying to survey all the relevant risks and downsides. But even if it does tend to be a pretty effective way of doing things, scaling up, doing it millions and millions of times seems very hard to accomplish.
Howie Lempel: It does sound like a logistical nightmare. And then I guess the other pharmaceutical that you hear a lot about are antivirals. Do you want to talk a little bit about what antivirals are and how they might help?
Greg Lewis: Sure. So, there’s generally antiviral agents, which impedes a virus’s entry into a cell or its replication, or its ability to assemble into viral particles. And generally, although I’m not sure whether we can call viruses living, it sort of interrupts or tries to mess up its life cycle, and so thereby hopefully stops it replicating and thereby helps the body eliminate it. As in most drugs, it often takes quite a while to develop something like this from scratch. So the main focus at the moment is basically just testing a lot of drugs, whether or not they’ve been used against viruses or anything, even infectious diseases, to see whether they show efficacy against this virus SARS-CoV-2. So they test this in the lab and they run clinical trials to assess whether these things actually bring clinical benefit. And I know many of these trials are ongoing. There’s some very early observational data reported from experimental use, but it’s still very early to say how effective any of these things may or may not prove. It’s worth saying, sort of similar to vaccines, even if you do find a drug which does prove to be highly effective – which would, I think, be a dividend of good fortune rather than good preparedness – how easily you can manufacture a lot of it very quickly might vary a lot.
Howie Lempel: So one thing that I’ve heard suggested, but I have no personal knowledge on this, is that to the extent that there were promising antiviral candidates, we’d be able to scale those up a lot faster than for vaccines. Is that also your impression?
Greg Lewis: I think it does seem very contextual depending on what precisely the vaccine candidate versus the antiviral candidate are. I can definitely see worlds where a given drug you can scale a lot more of than a given vaccine. After all, it may be the case that if it’s like a commonly used drug already for another indication, you may already have manufacturing capacity prepositioned. You might be able to scale that up, but it’s hard to give a very good general answer to that, or at least hard for me to give a very good general answer to that.
Howie Lempel: So I’ve seen some people, mostly amateurs, suggest that we should be basically manufacturing a lot of the promising candidates starting ASAP, with the knowledge that many of them are not going to pass through human trials because it would just be worth it to have already manufactured whichever ones make it through. I’m both curious if you have a take on that idea, and also whether people actually in the field of outbreak response have thought about this?
Greg Lewis: Yes, so I’m not sure of either. I agree on the face validity. Maybe a large question is the expected probability of a candidate which looks like it’s promising actually being good after all. So, medicine has many lessons to teach insofar as things which work well in animal models, tend not to work well in people, or often tend not to turn out to be so good in people. Things which show really good in vitro effects in basic science studies turn out to have no clinical benefit. And likewise, things which observationally seem to have helped turn out not to be helpful, maybe even counterproductive, when you put them into sort of a gold standard RCT. This sort of path: the genesis of evidence based medicine. And so, there’s certain barriers to that property whereby prepositioning, as in just making a lot in advance, is a good bet to make ex ante, and there’s others when it’s really not. I’d need to know a lot more on whether that’s a good idea or not, depending on a very hard to assess expected likelihood of success. So, I’m not sure. I’m not sure if anyone else has been doing this who would know more than me either, but I know enough to be uncertain.
Howie Lempel: And then I guess on a slightly different intervention, a lot of the sort of reporting and dialogue that I’ve seen recently has focused pretty heavily on the lack of ventilators at hospitals. And yeah, I was wondering if you could just this sort of like talk through that problem. How big of an issue is this? And why is it an issue in this case?
Greg Lewis: Sure. There’s been a lot of stuff I’ve seen, both by governments and also by the wider public expressing the concern of, well, if you have, let’s say, only so many beds in ICU or intensive care units, and a large number of people, a much larger number of people sorry, get very sick and need them, well what are these people who exceed the capacity going to do? And so one thing, is that we should try and expand the capacity of critical care services to try and make sure that people don’t go without potentially lifesaving medical care. And that seems right. That’s why lots of people are currently spooling all this up as fast as they can. One thing worth noting is although ventilators are very important, they may not necessarily be always the crucial factor or maybe sometimes even the most important factor in terms of how do you maximally surge your critical hospital care capacity over time to meet an expected surge of very ill people.
Greg Lewis: There’s a few remarks one could make. One is that even if you make a lot of ventilators, you still need people to actually run them and managing ventilator patients is not straightforward. So there’s a model, I think, from the society of critical care medicine which talks about how you could maximally increase staff by just basically getting staff who may have not trained in ICU as much to sort of help out. And they can get maybe one intensive care doctor who can cover like 96 critically ill patients. Normally it’d be much less, like one to four, maybe one to five. I don’t know. But it’s an order of magnitude, comfortably. I’m not an ICU doctor either, I’m afraid. But, the point is that even when we do this, this person has under them a lot of people helping them out, either being people who used to work in ICU or people who are sort of called in from outside.
Greg Lewis: And it’s roughly the case that you need sort of one highly trained person like a doctor or nurse, anesthetist or similar for every three ventilator patients. So, if you’re making, let’s say, a thousand ventilators a day, unless you can make or find 300 or so staff, who are particularly trained in using ventilation, you may not be targeting the most important bottleneck. We have seen in various scenarios, including in Wuhan, and I think also Lombardy, people using other measures which are sort of somewhat intermediate steps between ventilation and nothing, such as things like high-flow nasal oxygen or noninvasive ventilation, so things like CPAP machines or BiPAP machines, probably mostly the latter, which may also help. So, if you’re trying to maximally surge how you best manage a lot of very sick people who need some support for their breathing, it’s not necessarily clear you should fixate solely on ventilators as being the answer to that problem.
Howie Lempel: Yeah, so I guess you mentioned this equipment that’s sort of more of a middle ground that can help with oxygen that isn’t a full ventilator, so oxygen concentrators and CPAPs. Can you talk through, I guess, just what their role is? Are they likely to be able to keep someone out of needing a ventilator if people are put on those on time? To what extent should we think of those as potentially life saving equipment?
Greg Lewis: So I think we should. Maybe I’d like to put it in this way. So some people become critically unwell and who need ventilation, and that you can’t get around. And some of these other things, like noninvasive ventilation or high-flow nasal oxygen or other things like that, there is some initial data of this use which suggests although some of these people end up also needing to be ventilated as well, not all of them do. And obviously, it’s hard to tell whether that’s a causal factor, but I think there’s some RCTs on this for other conditions, which suggests this can, in a sense, rescue someone who would otherwise deteriorate further into ventilation, sort of keep them from not requiring it. I mean, there are other certain advantages insofar as they’re less labor intensive to manage as well, which is another plus, I guess.
Greg Lewis: And then I guess the tier below that is people getting supplementary oxygen by an oxygen mask. Again, this sort of supportive care for maybe severely ill people, but not critically ill people, is also very important because if they don’t have this, then they seem like a very large risk or a very high risk of further deteriorating. So, in a sense, although I’m sure everyone who’s thinking about this is already very well aware of this, you don’t want to fixate too much on critical care, because you actually, in a sense, do more to improve the mismatch between critical care demand and critical care supply by effectively reducing the demand by making sure people who are in earlier stages of disease get good supportive care so they don’t get worse, rather than trying to maximally increase how many ventilators you’ve got or whatever. If it’s the case that lots of people don’t need ventilation and could have been stopped from getting it, end up getting it because you’ve neglected these other aspects earlier on in the pipeline.
Howie Lempel: Maybe zooming out a bit before we change topics and start talking about non-pharmaceutical interventions. I guess I’m wondering, based on your overall take on the pharmaceutical and preparation pipeline, how optimistic you feel about efforts to delay the curve for weeks to months? Is your overall take that hospitals in the UK will be much more prepared for this situation one to three months from now, based on the stuff that we talked about, than they are today?
Greg Lewis: So I think it’s fair to say another benefit, as it were, so-called flattening the curve or trying to slow the spread or stop the spread, potentially. And it does buy you more time to spin up preparedness in a variety of senses. So I know in the UK they’ve started converting a couple of convention centers into major hospitals, for example. And so the thing is, the more time you get to do these things, the more time you have to manufacture relevant supplies and stuff, which seems to be definitely worthwhile. To give a crisper sense in this course of impression I’ll probably struggle, but it does seem like definitely an upside insofar as you can buy time. You can hopefully have more time for your surge to, as it were, surge and thereby have more ability that if things don’t work so well and you get many more patients than you were hoping to receive, then you might be better placed to weather the storm than if it’s day zero and you’re in this situation now.
Nonpharmaceutical Interventions [01:04:18]
Howie Lempel: So changing topics a bit from the pharmaceuticals. I think what I sort of got from the last section is we’re probably going to be waiting 12 to 18 months until a vaccine. Hopefully, in the meantime, we’ll be getting some help from antivirals, from preparing hospitals and training and better equipment. And then, there’s just sort of this question about what policies you employ in the meantime. So you had talked through a little bit about what are the non-pharmaceutical interventions or strategies that are on the table?
Greg Lewis: Yep. So to say this is a challenging environment is perhaps a mastery of understatement. So essentially, the options such as they are are these. If you do nothing at all, the modeling suggests maybe hundreds of thousands of deaths in the UK, and maybe 2 million or so in the US. The other costs of this event would be very hard to model, but probably also extremely bad. And this also may unfortunately be an underestimate. So it isn’t, to my understanding, factoring in further excess mortality which could be owed to hospital services being greatly overwhelmed. So your options to address this challenge are a variety of public health interventions, which are things like trying to improve people’s handwashing or sanitation or hygiene things. There’s options you can take around isolation or contact tracing. And there’s general social distancing as well. And the question of whether, when, how, and how much of these to use is, I think, the challenge lots of governments are currently grappling with as we speak.
Greg Lewis: But two broad strategies which have been described sort of basically determine what amount of these you implement at what stages, and I guess the overall objective. So the first broad approach is roughly along the lines of, we might call it mitigation or flattening the curve. And so I guess the overall objective here is, if you’ll excuse the term, a controlled burn of your population whereby, although you’re not really trying to stop how many people get the disease ultimately, you are trying to make sure not too many people get it at once and so your health services do not become overwhelmed. And you may also want to do things like, for example, ask elderly people to more strongly self-isolate because they’re at higher risk. And so you want to sometimes try and preferentially allocate, as it were, infections, both as a wider span across time, but also to those who are at lower risk of the disease. The principal challenge to this strategy is even if you do it pretty well, it’s not clear it will be enough.
Greg Lewis: So if you look at these sort of flatten the curve graphs everyone’s seen, the line for where medical services are is unfortunately not drawn to scale. And if you did draw it to scale, it’s much lower. And in fact, again, this Imperial report puts that pretty starkly. If you look… I think it’s figure two, but I want to double check. So even if you do surge capacity for medical services reasonably well, and you do follow these measures to do this degree of mitigation, you still end up with a number of very sick people substantially over your peak medical services capacity which obviously has a lot of human consequences.
Greg Lewis: The other approach which a lot of wealthy countries are taking, including the UK, and has been seen in places like China, Singapore and South Korea, is an objective towards trying to suppress. So in this, you are trying to stop people getting infected at all and trying to stop it for long enough that you can have a vaccine or similar which arrives maybe a year from now, and so thereby stop people from getting infected in the first place, and thereby lessen the overall burden of disease. And this, it seems, has roughly worked so far in various countries, i.e. places like South Korea or China. How they’ve done it has somewhat varied. But some mix of fairly aggressive contact tracing and some fairly aggressive physical distancing measures. And it has a very clear upside, if it continues to work.
Greg Lewis: The downsides of this various physical distancing and containment, although they’re more indirect are also unfortunately pretty substantial. So although it’s not like the economy would be working as usual if we weren’t doing anything at all, these probably have further impacts which are significant on economic activity. And although we don’t want to necessarily say like, “Oh, we just need to sacrifice lots of people to make sure the economy is booming”, we do know that economic hardship does increase people’s risk of ill health and death.
Greg Lewis: Also, of course, although people are keen to stress that physical distancing shouldn’t be social distancing, these things unfortunately do correlate to some degree. And so this social distancing or physical distancing impose some degree of social isolation, which plausibly has some unfortunate costs on people’s welfare. And then there’s lots more other side effects of having essentially everyone under a shelter in place order, for example, such as limited physical exercise. And unfortunately, I’m becoming aware of reports suggesting that rates of domestic violence are also showing signs of increasing in virtue of this. So lots of these public health consequences, which are not all good. And if you’re doing this for maybe a couple of weeks, you might reasonably enough conclude that these costs are outweighed by benefits, but the end game here is pretty uncertain. And you may have to continue with very rigorous measures like these for possibly months and months.
Greg Lewis: And one of the key challenges is that putting someone under a shelter in place order doesn’t immunize them from the condition. So, when you begin to relax these measures again, these people do remain susceptible. There’s a risk that as you relax these things, you sort of see the outbreak happening much like it would otherwise beforehand. So one hope is the facts on the ground change with a vaccine or a seasonality sooner than you expect, such that this interval isn’t so long in terms of the cost it’s accruing. Another one is if you get smarter at playing with all the sort of relevant levers of public health interventions you’ve got, so maybe augmenting some technological fixes. I know Singapore has pioneered a Bluetooth based contact tracing app, for example. Maybe other things like that which may prove worthwhile. You may be able to reduce the degree of distancing you’re doing, such that it’s not quite as onerous anymore, and so it’s worth continuing as a new normal for potentially a very protracted period.
Greg Lewis: Basically the two downsides are, one, it may not work indefinitely. If it doesn’t, you may end up not quite literally at square one, because you’ve got further time to prepare. You’re in a similar situation as you were beforehand, whilst having accrued all these costs. And secondly, these costs are extremely substantial, and so it’s reasonably uncertain to me as to whether if you weigh these things up, which option is better.
Howie Lempel: Got it. Thanks. That was a really helpful overview of the spectrum that people are talking about. So, I guess, one framing that you had on the suppression front, now I see how much you endorse this, it just sounded to me like you were saying the point of suppression is waiting for a vaccine or maybe antivirals. And so, you’re going to be in suppression for months to even a year plus. Do you think that that’s the most likely outcome from suppression? Or, I feel like there’s grown, very rapidly, a lot of support over the last couple of weeks for a strategy of suppression for some period of time. Then, once you’ve reduced the number of infected by enough, loosening restrictions, trying really hard to do contact tracing and doing that in an environment where you now have enough ventilators, kind of have those scaled up a little bit, and then just sort of like fine tuning the amount of distancing measures you need as you go forward? Yeah, I don’t know. What do you think about that? Is that basically your model of the suppression strategy or does that feel different?
Greg Lewis: No, that feels roughly right. It’s worth stressing that a lot remains profoundly uncertain. Essentially, people are embarking on public health interventions never before seen in human history. So, a lot is very difficult to work out. A nice turn of phrase I saw used actually by IDinsight in terms of what to do in poorer countries, was evidence-informed policy, because I think unfortunately no one has a very good evidence base to work with. So there’s the hope whereby we might just get progressively better at doing these sorts of things via various innovations with much more excessive contact tracing which might be really useful. We might get lots of really rapid point-of-care testing which might help. Maybe we should do temperature checks everywhere. Maybe something else, maybe something else. And maybe, if we add all these things in, this means we can loosen some of the more onerous public health measures we’re currently implementing.
Greg Lewis: But it’s unclear how much breathing room that will give you. It remains pretty uncertain. I mean, I think maybe a lot of data people are going to be paying attention to quite closely is… We’re seeing in various countries which have so far mostly, as it were, halted the epidemic: places like China, are beginning to loosen some of their restrictions which they previously implemented. And so, I guess, we’ll be seeing from their example, how far they can go and how successfully they can do this without thereby sort of getting back onto an exponential epidemic curve, roughly speaking. So the hope is, of course, that even if a vaccine is a while away, we get sufficiently good at this. We can do this in such a way which doesn’t have all the costs I iterated above about various measures, while still preserving this containment, but that remains pretty uncertain. I mean one sobering point is, again, this Imperial study did look at a model whereby you essentially feather the gas on very rigorous physical distancing measures based on your ITU caseloads. You can have sort of occasional holidays from very rigorous measures for a bit, but unfortunately, on their modeling, you spend most of the time under the very severe measures with occasional breaks, and not the other way around.
Howie Lempel: Anything else you want to say on suppression versus mitigation?
Greg Lewis: One thing which may be a particular cause of concern is how this will play out in poorer countries, which seem to have limited resources available to either suppress or mitigate, which looks, yeah, pretty troubling. There’s some papers which maybe we can link to on the program, talking about measures which poorer countries could take, but all the challenges we are currently facing in a country like the UK are all exacerbated with some further ones added in if it’s in a much poorer part of the world, which is unfortunate.
Howie Lempel: That makes a lot of sense. I even worry in the United States, when you start hearing talk about how suppression is going to be okay because we are going to have this dial where we can fine-tune exactly what the restrictions are, and so eliminate a lot of them until there’s signs of an emerging outbreak, and then bring those restrictions back and do contact tracing. I’m not so sure that the US government at this moment is going to be trusted to carry out that super complicated and novel policy plans that are high stakes. So, yeah, it’s scary to see what this actually looks like in practice.
Greg Lewis: Yeah. I think that fear should be pretty much held worldwide, to be honest. I mean, these things do seem extremely hard to implement, and I think it’s not unreasonable to say that some countries have fared better than others so far. How any of them will fare in the long run is very uncertain, and basically all the options you have to play with are some mix of extremely hard to do, uncertain to succeed, and have lots of indirect and direct costs. So that’s the unfortunate situation we find ourselves in.
Howie Lempel: We’ll talk a bit more about the epistemics of this whole situation later but one thing that’s been bothering me about this conversation is it seems like an enormous part of the conversation has been driven by one simulation study that came up with projections for how various distancing measures would affect the number of cases and the number of lives over time. And as far as I can tell, I’m not an expert, but my impression is that they’re one of the best modeling groups in the world, but I’m just not sure this is the type of thing that I can trust models to reliably get correct and I don’t know what’s going on behind it.
Howie Lempel: The model is supposed to be telling us what will happen when people do social distancing measures of the likes that have never been seen before so I don’t even know… Somebody decided that the parameter for that or the parameter behind the parameter for that was something. So I think the whole conversation just seems incredibly complicated and hard to follow and people are seeking an authority or a real source that they can ground themselves on and point to as true. I don’t know. It just seems very, very complicated and countries are going to have to make a lot of hard guesses.
Greg Lewis: Yeah. I would agree with, as it were, your counsel of despair with respect to how good the information do you expect to get. It’s worth saying that there’s been other people who’ve been modeling this besides the Imperial group who I have a very high view of. I think it’s fair to say that, speaking as a mathematical biologist, albeit one still in the larval stages, these things are very hard to do efficiently with lots of extrapolation for prediction based on, as you say, it could be sensitive parameters where you have very poor steers on. You can calibrate this somewhat by this melange of poorly observed and hard to interpret data you get from various sources to try and better calibrate you, but that’s very uncertain. I think all people who do the modeling stress that there’s lots of uncertainty attached and they’re certainly right to be so circumspect. Unfortunately, it may simply just be the best we’ve got. Because this is, to a large extent, quite a large leap into the unknown.
Howie Lempel: And my opinions on this are in no means made to insult the work that any of them are doing. I think it’s incredibly valuable. It’s just I feel bad about this situation where this is the best that humans can do right now since it actually is that hard of a problem.
What can you do personally? [01:18:25]
Howie Lempel: So moving onto another topic that comes up is we often have followers, readers, listeners who want to know, I guess, whether they ought to be helping out with the epidemic and what they can be doing. So I guess I’m curious about your take on stuff everybody should be doing to help, and then maybe stuff that certain groups of people can be doing to help out.
Greg Lewis: Sure. So given I was once a public health doctor, I should at least have some part of this podcast be a public health message. So typical recommendations to give everyone would very much be good citizenship norms of what typical governments are also recommending people do. And so these are maybe not in good order at the moment but it’s like, “Wash your hands regularly before having food, before going out, before coming back. Generally, if in doubt, wash your hands”. There’s a 20 second recommendation. There’s also a six stage hand washing technique you can look up if you really like. There’s also the respiratory hygiene issue of “Please don’t cough into your hands but cough into a tissue or, if worst comes to worst, inside your elbow or something”.
Greg Lewis: When it used to be relevant there was obviously “Please isolate yourself if you think you might be unwell, and don’t come into work when you’re sick”. Obviously now in many countries, including my own, the key recommendation is essentially this, which is to avoid all nonessential travel and avoid all nonessential contact with others. And the more people who do this, I expect the better things will be. So I struggle to emphasize it enough in terms of doing all of those things. Now, in terms of particular ways to help, I know 80K published,… Well a couple of days from me saying this, a post on if you’re mired to help, what you can do. I don’t have many obvious additions to this list. In terms of the question of whether rather than what, I would maybe strike some note of caution for a few reasons.
Greg Lewis: One is that this is probably now maybe the least neglected topic on the planet at the moment, and so the window for having a really outsized impact by being early, is closed. And this reason may be the case that folks that have prior knowledge or expertise in certain areas, there may not be very good things that they can do to contribute versus what they will be doing otherwise. Because for most, let’s say effective altruists watching this, there are still many other problems in the world unfortunately besides COVID-19, and those problems haven’t gone away. And so whether to switch from one to the other is uncertain. It’s also something I’m somewhat grappling with myself as I discussed earlier. So maybe but maybe not and maybe less so if you don’t have a relevant background which would make you well positioned to contribute would be my best guess.
Howie Lempel: That sounds right to me.
Greg Lewis: If you’re an effective altruist listening to this, it might be worth coming up with what your comparative advantage is versus the rest of the population in terms of trying to intervene on this problem. And it seems not to be that you find it important, because lots of people find this very important and so if it’s not that, and you don’t have a lot of relevant skills or knowledge to bring to the table, then there may not be lots of areas where you can contribute which has a really outsized impact versus the good citizenship or volunteering or the generally being a good citizen and things that people are trying to encourage at the moment.
Howie Lempel: Do you think that you might not have anything to do that’s much better than the good citizenship stuff?
Greg Lewis: Yeah. That sounds right.
Howie Lempel: So I also wanted to ask if there’s anything in particular that listeners might do but definitely should not be doing?
Greg Lewis: Yeah, so maybe some cautions I would express is a lot of people are looking at various ways of improvised medical care. Should I be trying to get some of these drugs to take for myself? Should I try and get this piece of equipment and so on and so forth. And I would recommend an abundance of caution with respect to doing these things. Doctoring yourself when you are a doctor is generally frowned upon and doctoring yourself when you’re not a doctor is probably even less advised. One of the reasons amongst many is medicine tends to be a very messy field where first principles don’t really get you as far as you would like. So you can’t just infer everything from first principles and be reasonably sure things will turn out alright if you follow them.
Greg Lewis: Now, I appreciate that some listeners might have a thought, “Well that’s fine for you to say. Maybe I’m in a situation where I can’t rely on getting prompt medical advice and care and I might have to improvise and surely I can do better than nothing if I’m not a doctor”. Especially if doctors like me, for example, start giving some helpful suggestions. And that might be true, but it seems like the best way if we wanted the medical profession to give some advice on improvised care would be a group of doctors who know much more than I do, who think about very carefully for offering recommendations rather than me offering some speculative ideas like maybe drug X is a good idea or whatever else.
Greg Lewis: I’m also particularly attentive of… As unfortunately we’ve seen fairly recently, people may take ideas people express like, “Maybe this drug might be a good idea” and do themselves harm by unwise use. And I think we’ve already seen some individuals tragically die through ill-advised chloroquine use, and I understand from Iran that many people have died of alcohol poisoning rather than coronavirus because of the mistaken belief alcohol consumption can be protective. So I can’t really tell people not to do things in all situations, but I would like to express that please check very carefully before diving in.
Reflections on the first few months of the pandemic [01:23:46]
Howie Lempel: On that note, maybe it makes sense to take a step back and reflect on the first few months of the pandemic more broadly. So one thing that I think really stood out was just the amount of real time information that was coming out and the speed of research and speed of information which I think has been really cool. It’s been really distracting for me at least as someone who does not actually work in this area. It also means that there’s just unvetted preprints going all over the place that non-experts can pick up and run with and sell. But experts are communicating with each other with really high bandwidth. I’m curious whether you have a reaction to that situation.
Greg Lewis: Yes, so I think on the whole, it’s been essentially a very good thing. And I think that both the pace, and amount, and quality of scientific research on this has impressed me. Things I’ve been particularly looking at have been the modeling studies. You usually get one high quality modeling study a day or more in the last couple of months. So it’s very hard for someone like me to keep on top of them, but that’s, I guess, a nice problem to have. And quite actually one thing maybe to take to heart is that genetic epidemiologists are just killing it at the moment because we have almost real time data of all the different virus strains out there. This thing called Nextstrain which seems like an amazing resource which we didn’t have in previous outbreaks, or previous very large outbreaks, which seems very valuable.
Greg Lewis: As you know, there have been some downsides of unvetted preprints flying around which may not always be the wisest. I think, briefly, I think maybe one of the most talked about preprints of all time, let alone with respect to condition, also which was happily, rapidly retracted because it was making gravely mistaken suggestions about how the viral protein of this thing can have some associations of insertions from HIV, which obviously got a lot of people thinking a lot of things.
Howie Lempel: That was a really bad one.
Greg Lewis: Yeah, and it was false. But happily the experts did quickly jump on and say, “No, no, this actually doesn’t make any sense. Firstly these apparent similarities are firstly not very surprising. Secondly, you’ve done some weird things about how you classify this thing which make it even more weird and doesn’t seem rightly plausible”. So that was good obviously. It wasted their time having to try and answer this which is maybe not so good. But I think if we’re taking the balance across the entire effort of the scientific community so far and this much faster, high pace way of doing things, it’s been also, I think, generally very helpful and needs to be welcomed.
Global catastrophic biological risks (GCBRs) [01:26:17]
Howie Lempel: Okay. So Greg, moving on to a different topic, I’m curious how the COVID pandemic that we’ve been discussing so far in this episode falls in relationship to the worldwide catastrophic biological risks that you spend most of your time working on?
Greg Lewis: Yeah, so one thing to say is global catastrophic risks or global catastrophic biological risks are sort of a term of art where it means something slightly different to… Presume which is like a global catastrophe, because like any commonsense definition of the term COVID-19 is a global catastrophe, but what we tend to have in mind when we talk about these things, are events of such large magnitude that they place the long-term trajectory of humankind in peril. There are a few different definitions of what GCRs are. That’s one. Open Phil’s one talks about how it could globally destabilize enough to permanently worsen humanity’s future or lead to human extinction and you get things along these lines. So it’d have to be like extremely, extremely bad events. And so I don’t think any pandemic in human history has ever really got to that sort of level: so things like the Black Death, or 1918 influenza or things like the Justinian plague I also don’t think other major current health crises at the moment would also count as these sorts of risks. So, for example, I don’t think antimicrobial resistance is a GCBR, nor HIV/AIDS and so on and so on and so forth. None of which is meant to say these things are trivial or they aren’t important or anything along those lines. But it’s to sort of give a sense of what I have in mind, is events of a greatly different order to these undoubtedly extremely severe threats to global health. And so given COVID-19 falls in this set of very severe threats, it nonetheless doesn’t rise to the level of a threat to human civilization, which I guess you can consider reassuring, although it’s obviously not much for reassurance.
Howie Lempel: Yeah, that sounds right. It certainly is somewhat reassuring to hear that like this is not, you know, one of those real worst-case scenarios. I guess GCBR still feels to me like a very high level concept, but I don’t feel we’ve quite described exactly what one might be. Do you want to talk through what are the types of GCBRs that you might worry about and sort of use that as a lead in into talking about, you know, how likely are they, how bad are these things?
Greg Lewis: Sure. I mean, it’s worth saying that how bad an event needs to be to threaten humanity’s future is a pretty uncertain question itself. And so for this reason, where you, as it were, put the bar for how bad an event must get until you start being worried about a threat to civilization as a whole, is a very uncertain one. I mean one rule of thumb often thrown around is like, “Oh, if something kills 10% of the world’s population” then it starts getting into the category where you start getting very worried. I mean obviously events like that you’d be worried about for all sorts of reasons, but if you’re worried about this threat to the future, you still begin to think events at like ten percent or higher might pose very grave danger, not just people like, “No, but obviously you could live forever after”.
Greg Lewis: So I’m not saying that like, as it were, proportional mortality is the key or only criteria which one should be using, but it’s actually very hard to figure out what those should be. So, with all that said, we can maybe, for the purpose of argument, just think about, as it were, very bad biological events and see well, could these get even worse to the degree where you start getting really worried? So one example would be like, could there be a naturally arising event which is even worse than we’ve seen so far. So something even worse than let’s say the Black Death or the plague of Justinian or the 1918 influenza.
Howie Lempel: And can you give us a sense of how bad those were?
Greg Lewis: Sure. So a run down of these would be, it’s worth saying these are also uncertain because you’re trying to often maybe work out what happens like hundreds of years in the past or longer. And so it can be hard to tell exactly what happened when, or how severe these events really were. But anyway, such as they are, the plague of Justinian happened around 540 CE, probably it arose in Asia before spreading around to the Byzantine empire. There are estimates that said it killed 6 million people or 3% of the world’s population. And they’ve had various historical consequences of various powers which are present at the time. It’s worth saying there’s a caveat to this in that there was a recent paper published, I think, last year, suggesting it may not be as bad as previously thought, because if you look at the archaeological data of various types, you don’t see this very large discontinuity which would fit with like a certain disaster happening in this part of the world. With that being said, then there’s the Black Death which everyone’s heard of, which maybe killed 275 million people. Maybe 10% of the world’s population, although it’s very hard to say. And maybe we’re still trying to figure out what impacts that had on European history.
Greg Lewis: Another couple which may not be as well understood or well known to listeners, would be what’s called the Columbian exchange. This wasn’t really a single event, but probably a succession of pandemics brought by European colonists which then devastated Native American populations. It’s very hard to work out what proportion of people died. It might vary a lot, but it was probably extremely worrying. You get figures like 80% of the population of various native populations over the 16th century, probably. Well, at least partly, maybe substantially attributable to infectious disease. And then there’s the 1918 influenza pandemic, which globally maybe killed 50 to 100 million people. Probably more than either World War. So these are all obviously extremely large and extremely bad biological events by any sort of reasonable definition.
Greg Lewis: That being said, it’s sort of still hard to see how you would get from an event similar to these, to something which does threaten human civilization as a whole. Maybe the key challenges is that, well not challenges, but one of the causes for reassurance is that these things typically affected one part of the world. So these Eurasian and American populations were fairly separated, so the thing which affected one did not affect the other. Even events which had reasonably high global death toll and then did spread fairly globally like the 1918 flu had surprisingly limited historical impact relative to either World War each side, probably killed fewer people than the 1918 flu pandemic did. So that being said they are, as it were, proof of principles, you can begin to approach this level where you start getting worried via like naturally occurring events, roughly speaking.
Greg Lewis: And then there’s the question of… Another point to make is if we’re worried about extinction risks, you do have this argument which I know Toby Ord talked about a lot in his book The Precipice , which is if you survive for a very long period of time, then the risk of something which sort of stops you, is quite low just based on this track record and there’s some anthropics here, but it basically all factors out to be mostly right. And this probably also applies to these events. The key challenge is things obviously have changed in the last century and the last few hundred years, which can increase or decrease the risk of diseases or emerging natural pandemics being worse or better than they were beforehand. And there are reasons either way and whether it’s like we’ve gotten more or less vulnerable compared to like say, 200 years ago or 400 years ago or whatever. Obviously the risk factors are things like climate change, having very large animal reservoirs which you’re making for meat or similar and also lots of international travel and trade.
Greg Lewis: On the other hand, of course we are now in receipt of various medical interventions. Obviously as I discussed earlier in the program, these are not always straightforward to implement but they are at least possible to do which were impossible if it was happening like 250 years ago. People probably now are typically healthier, there’s better sanitation, hygiene, and all of these things seem to be protective factors. So how one ways these things up versus like overall risk of a very large event and how soon that might be, is very uncertain. I might still guess, despite being in the midst of a pandemic at the moment, that the risk may have gone down. But these events are so sparse, it’s very hard to work out what the rate is or whether it’s going up or down either. And we also have seen, in terms of endemic infectious diseases, these have steadily fallen in terms of their burden of disease for humankind over the last few decades.
Greg Lewis: Obviously how well we can translate that into risk of sudden shocks of very large outbreaks of disease is very uncertain. So if you weigh all these things up, my best guess is that there’s not no risk of global catastrophic biological risk from this, but I think it’s like hopefully declining and probably reasonably small risk because I guess if that’s true, the question’s like well, what’s the most severe one? And what I’m typically worried about, or more worried about roughly speaking, are events which are in some sense human caused or anthropogenic. So maybe the reason why I’m all worried is a couple of things. One is this track record story, which I discussed earlier about how we’ve managed this long without dying from a natural pandemic, so we probably won’t die in the next 10 years. You don’t really have that when our entire understanding of biotechnology only really spans 100 years or maybe slightly more.
Greg Lewis: And I think there’s also… Although it’s hard to work out how you price these in, there are some direct object level causes for concern. I’ll give maybe three. One is that we now have the ability, and it has been used to produce from scratch, in the lab, infectious agents which cause some of the most most dangerous diseases in human history. Like people have reproduced from scratch the 1918 flu virus for example. There’s obviously a risk if this ends up getting misused or you might have the risk of repeatedly rerunning the worst biological events we observed in history so far. There’s also a risk that we may either inadvertently, or on purpose, do worse than nature has done. So nature may not prove an unsurpassable biological terrorist, and there’s a risk that thanks to advances in technologies, humans may be able to do things which are not seen in nature and even nastier for what we see in nature, which is obviously another cause for greater concern. There’s also this general feeling, looking to the point I made earlier, where a lot of biotechnology is fairly hard to predict and fairly hard to forecast.
Greg Lewis: I mean, in the words of Drew Endy, most biotechnology has yet to be conceived, leave alone made true. And so in this large territory of unknown unknowns, it may be optimistic to presume there are only familiar dangers. So all of these make my concern focus more on human generated events using biology, in some sense, rather than dangers arising through the natural world itself.
Howie Lempel: Got it. And then within the category of artificial risks, it sort of spans over a lot of different scenarios. So there’s accidental and deliberate risk, where “accidental” might be a scientist working on a project that might be beneficial, in expectation, but who releases a dangerous pathogen while doing it. Deliberate would be like releasing something on purpose to do harm. And then within indeliberate, there are ways that you can break that down too. But yeah, I’m curious like where you think most of the risk is coming from within the artificial category.
Greg Lewis: Yeah, so I’m obviously always deeply uncertain. It’s very hard to give a good guess on risk share. I’m not sure whether I count as an expert, but I mean even people who are experts would struggle to have great confidence or resilience in their predictions. Nevertheless I will give it a go. So one of the challenges which actually may be something we come onto later are reasons maybe not to be so worried about this area, is that we haven’t really seen many events which have been human caused which are similarly bad to naturally arising events like the typical death toll from scientific accidents or by bioterrorist attacks or anything else. It’s comfortably less than most other infectious diseases at any given year. So you’re often trying to weigh up within this, which seems risky given the lack of a track record.
Greg Lewis: And there’s also, I guess, another annoying philosopher’s point whereby the distinction between accidental and deliberate isn’t perfectly crisp. So you can imagine a Dr. Strangelove scenario where someone deliberately makes something very nasty but then another agent uses it without authorization: so it’s the unauthorized use of something that’s deliberately made, but that’s somewhat an accident by light of the person who made it in the first place. Or there could be a thing whereby someone makes something very nasty and accidentally deploys that without intending to. Which again there’s this mix between… Well, you’re deliberately making something very bad, but you weren’t deliberately like releasing it to cause harm. So that’s like a small point. But in terms of the general sketch. One expectation, well hopefully is one expectation is, there are more people who are well-intentioned than badly intentioned, so maybe there’s a higher rate of people who have good intentions who then make mistakes versus people with bad intentions doing these deliberately.
Greg Lewis: That being said, if you’re trying to cause a very, very bad thing to happen, you’re probably more likely to achieve it. Trying to do it deliberately rather than doing so by accident. But all of this is deeply uncertain. The evidence I’ll offer in favor is conjecture: is if you look at other things in terms of single event casualty counts. Maybe one comparison would be, for example, motor vehicle accidents. So most of those happen by accident, and there are far more accidental deaths from cars, roughly speaking, than people deliberately using cars kill each other. But if you look at something like the largest casualty events involving a car or indeed a plane or other things, you see that most of these are from deliberate acts of misuse. So unfortunately, vehicle ramming attacks, for example, tend to have a much higher average death toll than the typical car accident, even though there’s many more car accidents.
Greg Lewis: There’s some very loose evidence I’ll induce in favor of this idea, that if you’re looking at very severe events maybe, or very large scale events, you might notice higher prevalence of those which come from deliberate bad action rather than people making mistakes or making accidents. So for that reason, although that’s very tentative, I’ll lean in favor of thinking there’s more of a danger from deliberate misuse, all things being equal, than from accidental misuse, roughly speaking.
Howie Lempel: Got it. And then when you think about deliberate misuse: by whom?
Greg Lewis: So there’s unfortunately been a not-so-long but fairly dark track record of people trying to misuse biology to cause harm. So various terrorist groups have tried at various times to do things. Various individuals have used biology for criminal attacks or trying to murder certain people. And there have been, unfortunately, several very large state biological warfare programs over the course of the 20th century.
Greg Lewis: So weighing up which ones you should be most worried by is a little bit tricky. I did a little diagram noodling, I guess, in the problem profile, giving sort of one model. But to give like the sort of considerations I’m attending to. Maybe one point is that typically more sophisticated actors will probably get to a given dangerous misuse possibility before. The less sophisticated ones, they probably are the vanguard of a risk. But as we typically observe, the barriers to entry of any given technological capability go down, then you might have a much larger pool of less sophisticated bad actors who may also have access to it. And so how you weigh these things up is a little bit uncertain. I mean, I guess one thing you might say is that you might worry more about more sophisticated actors to start with, and as time goes on, maybe your risk share begins to move from more sophisticated to less sophisticated as time goes on.
Greg Lewis: Although hopefully, you close the risk window sooner rather than later so you stop that transfer happening or hopefully stop it altogether. But that unfortunately can’t be guaranteed. So as far as it goes, I guess I’ll maybe lean towards more sophisticated actors versus the less sophisticated ones, but again, as always, it’s very hard to say.
Howie Lempel: How decision-relevant does that end up being?
Greg Lewis: It can be. It’s like one of a very large cloud of considerations you want to try and weigh up as best you can. So it’s not completely irrelevant. Some things obviously aren’t really selective between one or the other. But other things can be. And insofar it goes, you do want it to try and have some steer on this in terms of making decisions.
Howie Lempel: So I guess one question is why a state actor would ever use these? Like when you compare them to other WMDs, I mean, these don’t seem all that effective. The fact that you can get your own people harmed seems like a major disadvantage. So what are the reasons someone would use this?
Greg Lewis: So there’s a variety of possibilities. There’s at least some prospect where use of disease as a weapon may prove an attractive addition to a state’s pre-existing portfolio of violence for a variety of reasons. One thing often said in the literature is that biological weapons are like a poor man’s nuke. So it’s like a strategic deterrent which isn’t as good as a nuclear weapon, but it also somewhat does the job in terms of deterring people from attacking you. Whether in fact it can do this, or whether in fact states who pursue biological weapons are trying to do this, is like an active source of controversy for all sorts of reasons which perhaps are better explained in my profile than verbally now.
Greg Lewis: There’s also a point that even if states wrongly perceive them to be useful, they may still do it anyway. States are not always perfectly rational in all respects. And obviously historically, we have seen states, in fact, pursue industrial scale biological weapon programs.
Greg Lewis: Now whether that was, in a sense, strategically rational for them to do so may be open to question, but obviously the fact that they still do it, still causes a lot of concern.
Howie Lempel: I guess one thing that might be reassuring is it seems like states have even less incentive to acquire biological weapons that could potentially cause GCBRs. Is there any history of states pursuing weapons of that scale?
Greg Lewis: So one story is, I think, states have pursued, or as best we understand… All these things are very hard to interpret because typically these things are held in close secrecy for obvious reasons. But historically, we have seen states pursue the use of these weapons with mass casualty purposes in mind, which obviously is a cause for major concern if they ever do this again.
Greg Lewis: Another thing to say is, I think it’s fair to say that states often do not have perfect control, like a principal-agent problem with respect to what their highly classified and deeply secretive enterprises may end up doing. So even if the state only wants one particular thing they want to do with the biological weapon, it may be the case nonetheless that the program itself just does things unauthorized which would also be a cause for major concern as well.
Howie Lempel: That makes sense. And simply moving away from state actors, on the non-state actor side, something I’ve always been a little confused about is just why we’ve seen, I guess this is my opinion, so little bioterrorism so far? And when I used to talk to global health security folks about potentially working on bioterrorism, the response I sometimes got was just like, “Look at how few events that we have of these per year. Look at the number of deaths being caused by endemic diseases. Why focus on this”? Yeah, so what’s your thought on that?
Greg Lewis: Yeah, so it’s definitely fair to say that a lot of the motivation for GCBRs in general, and also where I assign my risk shares, or where, obviously I guess people should assign their risk shares, is predicated mostly on, as it were, betting against the track record, or trying to go, “Oh, I think this changed markedly due to this fact”, which is not a very resilient form of argument.
Greg Lewis: In terms of the track record, it seems fair to say there have been mercifully few bioterrorist attacks which have caused mostly little humanitarian damage or consequences. That said, various terrorist groups have attempted to pursue biological weapons in the past. Al-Qaeda, probably ISIS, and Aum Shinrikyo, may be the most prominent amongst them. So it’s not necessarily for lack of trying they haven’t been able to do this.
Greg Lewis: Either fortunately, I hope this doesn’t change, but biological weapons prove much easier to say than do for all sorts of reasons. There’s a very good book called “Barriers to Bioweapons”, which illustrates a lot of the challenges. The worry I have is it’s not maybe a cast-iron guarantee that these barriers will remain as high as they’ve been so far. Obviously if a barrier goes down, then maybe there’s more of a prospect of something very bad happening, such as terrorists trying to use these sorts of things.
Counterarguments to working on GCBRs [01:45:56]
Howie Lempel: Yeah, so I guess so far we’ve talked mostly about reasons to think that the scale of this problem merits attention from longtermist EAs. Are there good reasons that a longtermist might look at this problem and given some reasonable set of beliefs, decide that the scale just isn’t competitive with other areas?
Greg Lewis: Yeah, many. So there’s a lot of uncertainties here as I’ve said, I’m sure, throughout this podcast, but one more for luck. So a few uncertainties would be that there’s quite a lot of uncertainty about, as I alluded to earlier, well firstly how big an event must be to risk civilizational collapse, and also, even once human civilization has collapsed, how likely it would be to recover fairly well.
Greg Lewis: Now obviously one would probably prefer not to have civilization collapse on you, but there is a story whereby actually maybe humanity proves very resilient to even extremely large catastrophes. So even if you ruin the current civilization, despite its profound humanitarian costs, it may be the case that given a few hundred years, things will have mostly recovered back to normal and you wouldn’t be much worse off than you started with, and the future is still in play.
Greg Lewis: So in other words, even events which cause massive scars in humanity’s past may not ultimately greatly harm its future. So that’s one broad story you might have. So if you think, for example, that collapse is no big deal, or collapse is reasonably unlikely in the first place even with very large events which threaten collapse like this, then probably relatively less weight should go on those versus maybe things which are fairly exclusively extinction risks in their own right. So something like AI perhaps is the most commonly cited version of this.
Greg Lewis: So that may be one of the key uncertainties. Then a lot of the other things would be more issue specific. So a lot of the motivation for this relies on fairly non-resilient first principles arguments, which I’ve previously objected to in other contexts, of trying to adjust what we’ve seen so far which is reasonably reassuring and saying, “We think it’s going to get much more dangerous in the future.”
Greg Lewis: That’s unclear, you could argue quite a lot about how plausible that would be. But that’s the essence why many experts in adjacent fields aren’t hugely persuaded by this as a grave and high priority danger.
Howie Lempel: Got it. So going back to the recovering and collapse bit, I feel like this actually comes up pretty frequently as one of the canonical open questions in longtermist EA. Do you happen to know if there are… Is there anything that you would tell someone to read if they wanted to get more informed on this? Or do you know if there’s just people working on it?
Greg Lewis: So I’m not sure of a good canonical source, I think I picked up most of my limited understanding just by being in the right water at the right time. I know there are people who are working on this. I think some work is hopefully coming out some time soon. But I hesitate to break anyone’s confidence just in case that’s meant to be kept–
Howie Lempel: That’s reasonable.
Greg Lewis: Yeah, so I think it’s more like “Watch this space” is best as I can tell. Maybe some of your listeners may have better recommendations for that.
How do GCBRs compare to other problems? [01:49:05]
Howie Lempel: Then I guess, stepping back and summing up overall how much of a risk should we think of when we think about GCBRs? Do you think that it should be at the top tier among areas that EAs think about?
Greg Lewis: Yeah, I’m obviously biased given what I’m working on. But yeah, I think it could be argued to be roughly in the top tier. It’s worth saying actually, in terms of this, that maybe the principal… Well one of the main discussions is how to weight it up versus AI? Because AI, at least in my impression, seems to be like a bigger risk. Bio seems more neglected in EA land but maybe not in the wider world. So it’s quite hard to weigh these things up.
Greg Lewis: So my best guess is bio should be a relatively more junior member of a portfolio compared to AI. But maybe relatively more senior compared to other particular things with respect to catastrophic risk generators like nuclear weapons, for example. That’s obviously a very non-resilient view. That’s my best guess.
Howie Lempel: Yeah, so now that we’ve talked a bit about the scope of the problem, I find it really challenging to think about how neglected GCBRs are. And we know that the US is already spending billions of dollars a year on health security which just makes this space a lot bigger than most of the other ones that longtermist EAs look into. So how do we know that there are still good opportunities?
Greg Lewis: That’s fair. I also struggle to work out how neglected this area is, but I still think there are useful ways to contribute, and I’ll try my best to give an argument as to why. So there’s obviously a reasonably straightforward point that you can spend billions of dollars on something and yet it still be neglected from the point of view of the universe. Billions of dollars are spent on global health, on climate change, and other things besides, and we still probably think, compared to the optimal allocation, probably more should be done.
Greg Lewis: So you can still be neglected qualitatively despite that. It probably doesn’t get you very far, because you obviously want to work out to what degree are these things neglected? And so you want to have maybe a better sense of that. Another thing you might say, where given things like global catastrophic risk in general, or other things like global public goods, and these rare events, they principally affect future generations which generally have a natural constituency. You would guess these things tend to be poorly provided for by either governments or markets or similar things like that.
Greg Lewis: It feels like another reason for having a good impression, from the first principles of this area, probably would be neglected: it doesn’t tell you how much still. There is some tentative work looking at things like pandemic preparedness, suggesting that certain things could be very cost-effective in terms of their reduction of extreme events.
Greg Lewis: So there’s modeling suggesting that the typical flu pandemic mostly pays for itself in terms of the very severe events which you occasionally get versus the typical one. There was suggestion, I think, from the World Bank that various interventions towards One Health, which is a mix of public health and animal health, and trying to cover the two amongst other things, and environmental health as well, could reduce the risk of emerging pandemics by some fraction that could have a very good rate of return.
Greg Lewis: So those are all, I guess, general points one could make. It’s a little bit hard for GBCRs to give really crisp top 10 best buys. But I can give a few which seem to be promising. And although it’s not just a matter of money in terms of how to make them better, these do seem the area which seem not so horrendously hard to work on you couldn’t make progress. And it seems a shame more progress isn’t already being made.
Greg Lewis: So a series of examples, more on the technical side, which mostly correspond to what Cassidy Nelson talked to you guys about in terms of technical innovations, like better sequencing based surveillance and things like that, which seem to be extremely promising and could plausibly help a lot, especially with pandemics arising from things you haven’t seen before rather than things you already have seen before and got tests developed for.
Greg Lewis: So I’m probably not going to do any better than referring to her podcast, but all of these seem to be things which are not impossibly hard to do. They are to some degree not yet ready to go, but getting closer and closer, and these things could be accelerated, and if we did, I think it would be a great benefit. These are, I guess the way of the future; I guess recent events unfortunately demonstrate our future is already overdue. That’s one broad area. where there’s various technical things you can do which don’t seem wildly costly and still seem, A) tractable, and B), neglected.
Greg Lewis: On the policy side I would suggest things like our management of Dual Use Research of Concern and the Biological Weapons Convention as a whole, are perhaps emblematic of neglect which shouldn’t be there. So there isn’t a neat single trick to fix this, although I’ve got some ideas on how you might incrementally improve things. But the challenge whereby, for example, in Dual Use Research; DURC is Dual Use Research of Concern. So this is research which although it’s well intentioned, it could be potentially misused either accidentally or deliberately to cause harm.
Greg Lewis: So this often comes up in terms of so-called gain of function work, where we’re trying to get maybe a pathogen to do something which it couldn’t previously do. And depending on what that thing is, that could be very concerning. So there’s a challenge whereby… there’s many challenges. One is that if a given funder, or a given journal says that this work is too dangerous for us to fund or to publish because of its risk of being misused, there’s not very much to stop a practitioner who thinks they’re doing the right thing shopping around between several.
Greg Lewis: And you end up with essentially what’s called a unilateralist’s curse whereby the decision-making here defaults to the least risk-averse person of the group. So as long as one person thinks it’s a good idea it will happen, even if everyone else thinks it isn’t a good idea. And that seems not to be the rule you want to have with potentially things which could cause a major pandemic if they go wrong.
Greg Lewis: It seems like so much could be fixed. Well maybe not fixed, but improve better coordination, maybe some better governance mechanisms such as you could imagine taking something from export control regimes where they’ve also got no undercut rules. So if one country said, “We’re not going to export that to this country, or to this individual or whatever”, all other countries that are a member of this group also agree not to do it, even if they personally would’ve done it if they were asked first. This means you’d now default to the first person you asked rather than whoever happened to say yes, which is slightly better.
Greg Lewis: And these things are not easy to set up. They do not strike me as impossible. The other example is the Biological Weapons Convention. So Toby Ord’s mentioned this in his book; the BWC, which is the treaty which almost all countries have signed up to which prohibits them from developing, using, stockpiling, basically having anything to do with biological weapons. That has a staff of, I think, four people, maybe three, I can’t remember. And a budget less than the typical McDonalds in a country like the UK.
Greg Lewis: Again, it’s not like you can just mail these people a cheque and you just fund the BWC that way. But it seems to be indicative of, given the dangers which this poses, you probably want to do more, or as much as you can to further strengthen the norm against biological weapons use. To have further international dialogue about the dangers of emerging biotechnology and how the threat and its misuse can be best mitigated.
Greg Lewis: And it seems like further capacity for the BWC, although much easier said than done, could usefully contribute to reducing risk of things I worry about. And these problems, although they are not easy, they seem somewhat less hard, for example, working out how you’re going to manage transformative AI capabilities.
Greg Lewis: So I would take the aggregate of this: a first principle argument which suggests that we should expect it to be neglected. Some evidence of potential high impact things to do, and some suggestion there seems to be gaps in the market as it were, would lead me to suggest it’s sufficiently neglected that I think people can usefully contribute and it could be one of the most important things people, particularly those who care about the long-term future, can contribute towards.
Howie Lempel: Got it. And then I guess as people are making career decisions, I think one factor that often comes up is if they’re longtermists and if that’s your motivation for being in the field, they’ll often really want to work on projects where they will be directly working things where the story for how it’s important to the long-term future is really clear. And so I’m curious about your take of how much of the broader health security sector or biosecurity and pandemic sector seems like it would be useful for mitigating GCBRs in particular? And how well targeted is it?
Greg Lewis: So I think there is at least a broad convergence between what you might call status quo or conventional spending in health security, biodefense, biosecurity, et cetera, and what you’d want to do if you were trying to reduce GCBRs. Things which help for smaller outbreaks or smaller acts of misuse also typically help for larger ones. And although these things might subtly differ, so the disease surveillance system I would want, trying to purely avert, or for argument’s sake, purely avert long-term risk, might be slightly different from the one set up with more conventional priorities. They would overlap substantially, and so work in this direction still correlates pretty well with the things I’d want to see.
Greg Lewis: This isn’t going to be perfect, and it’d be very surprising if it was. As I think there are things one could do which either complement the existing portfolio to better address these very large risks I worry about. Or things which could be done, in addition, alongside it for example, which could also contribute as well.
Greg Lewis: I would typically favor the former thing, versus the latter. Mostly because there is so much money and effort already spent in this area. If you can usefully complement or reallocate what is already going on, you might have a very high factor of leverage in terms of how much activity you’re shifting towards better ends than if you were trying to plough your own furrow, doing your own work.
Greg Lewis: My typical guess is people are often better placed working in existing fields with existing stakeholders to try and contribute that way, rather than going out on their own. So I guess almost a corollary of this is the folks who are just starting out, I often feel it’s like they’re often well-advised to try and get career capital in areas which are adjacent to the problem, rather than trying to become an independent GCBR mitigator or whatever you might want to call it.
Greg Lewis: The reasons for this is that not only is there like a lot of leverage if you begin to work for an existing stakeholder, but often a lot of the skills and knowledge you would need to understand the field and usefully contribute would be contained in existing bodies of knowledge and expertise, and you’d probably have a better way of getting access to that by entering them rather than trying to pick things up. It’s very hard for anyone in this area to know everything, but having a home discipline where you know the lay of the land, which you then can apply to problems of GCBRs typically seems like a pretty good strategy for most people in most cases. That’d usually be what I’d recommend.
Careers [01:59:50]
Howie Lempel: Okay, so if we have listeners who basically buy the case that this is a particularly promising problem to work on, and are considering it for their careers, how should they be able to tell if they are a good fit? What makes someone a good fit for the area?
Greg Lewis: Yeah. I’m not sure if I count as a good fit myself, but I may have a better idea of what it looks like. So I think perhaps one of the assets folks who want to make a difference would have is having a sense of prioritization towards the long-term future. That’s not to say that people can’t usefully contribute who don’t have this: many do. And it’s also not the case that folks who don’t have this, who don’t share this moral conviction should rule out working on the broader area of health security.
Greg Lewis: It may be something which people interested in global health, for example, might find a way they can usefully contribute. But that’s still quite a long way out of my area. With that being said, I think there are a few aspects to this area which make it somewhat distinct from typical areas where EAs might be involved in, which might influence whether they think they have a good fit to this area versus others.
Greg Lewis: So one area which I think is worth stressing is this is a fairly delicate and fraught area in a variety of ways. So it’s not really a move fast and break things sort of field. So there’s a few reasons for this. The first is insofar as part of the concern here is about acts of deliberate misuse, there is this information hazard aspect to it, whereby giving bad people good ideas could be very bad in itself. And so there’s some degree of caution around probably it’s a pretty bad idea to blog the top 10 bioterrorist attack strategies current bioterrorists aren’t doing. Or similar things like that.
Greg Lewis: That’s a very obvious example, but unfortunately things can get a little more subtle than that in a variety of ways. Another reason why the area is delicate is although GCBRs are fairly new as a term, nearby issues have been around for quite a long time and they intersect with lots of fairly well worn disagreements or conflicts both between expert communities, like science versus security, and also between state actors, industry, and other things besides. And given you can’t usually implement solutions yourself, you have to try and build up coalitions of support, this generally urges towards some degree of caution before alienating certain groups, saying things out of turn, and so on and so forth.
Greg Lewis: I think this applies to a somewhat lesser extent in so far as EAs joining an existing biosecurity community in itself. I think it’s fair to say that the past track record of a group of people who are smart and who care and are enthusiastic trying to team up with a group of people who have been working on this for a long time hasn’t always gone extremely well. And happily so far in bio it’s worked great, and I’m keen to see that continue.
Greg Lewis: So the upshot of all of this is that this is an area where discretion is a particular virtue, moreso here than other areas. And so folks who are willing to do this, this may cash out in the sense of maybe talking to peers before going off and doing something on their own, maybe checking with others, maybe willing to defer to consensus, even though personally it sounds like a really promising idea. Other people are expressing caution: maybe it’s worth holding off at least until you get clarity in the agreements and things like that do, I think, seem to be pretty important in terms of navigating this area and not hitting into hidden traps which can be very hard to see.
Greg Lewis: I think another aspect to this area is there is quite a lot of pre-existing expertise, if not in GCBRs qua GCBRs, but with respect to all the things that GCBRs might interact with. So, for example, when I occasionally attend expert meetings, the people in the room who’ve worked on public health preparedness have done so longer than I’ve been alive. And I think I’ve got three degrees now; I think that’s about right, and have gained relevant experience over the last 10 years, and I’m sort of roughly par for credentials and below par for experience with respect to the typical people I end up working with in this area.
Greg Lewis: This is not just a “do your time, pay your dues” sort of moral. I think it’s partly owed to the fact that there’s a lot of stuff to learn. These are also very messy areas somewhat like COVID-19, in fact. And so it obviously requires quite a while to gather relevant knowledge and a tacit background of what’s going on. And so for these reasons, trying to gather relevant terminology is very valuable, often with further study or further experience professionally, or in graduate school. There’s also the point that given there’s often a premium paid getting an advanced credential of some type, whether it’s a medical degree or a PhD or similar, in terms of being able to take, especially with existing stakeholders, prominent high impact positions to reduce risk.
Greg Lewis: So if you’ve already got them, then so much the better, but do bear in mind there might be quite a lot of time one might have to spend in terms of tooling up before one can make lots of really important contributions. Another thing to say is insofar as a lot of this work is based in a national government, your nationality, unfortunately, can be quite important in terms of the opportunities that are there. Depending on basically what your country’s already doing with respect to how usefully you want to contribute to it. That also may color how attractive one finds this area because the opportunities may vary based on a UK or US system amongst other things besides.
Howie Lempel: Got it. And then is there an academic background that would make someone a good fit or not such a good fit?
Greg Lewis: So people who end up working in this area, either under the heading of working on GCBRs or they work on areas which are important for GCBRs, but don’t call themselves working on GCBRs itself, their backgrounds vary a lot. Because these areas are not quite pan-disciplinary, but they do cover a lot of different things. You could loosely subdivide it as more policy versus more technical areas. Obviously, there’s also potential technical things you might have to contribute, things like synthetic biology, bioinformatics, many other things I’m neglecting, probably like people who are subject matter experts, in particular pathogen types or species may also be relevant, depending on what you are worried about, and so on and so forth.
Greg Lewis: There’s a lot of different backgrounds there which can be relevant. And then on the policy side, people often contribute from a variety of areas. From science and technology studies, to international relations, to biodefense to public health – although that can be technical as well. So what I may not be describing very well is a large range of academic backgrounds could usefully contribute, or could usefully deploy anyone who wants to contribute to this area.
Greg Lewis: Obviously which parts you probably end up contributing to would depend on your academic background to an extent, but it’s not very crisp like you must have a PhD in X to do useful work here.
Howie Lempel: Is there any sense that if you don’t get one of a certain number of degrees you’re just going to hit a ceiling at some point?
Greg Lewis: I think it’s pretty contextual. I think it is notable when I look at various quasi-academic groups in this area, you can sort of tell, bluntly speaking, someone’s rank by their degree. So many places… Like all their directors have PhDs, all their staffers have Masters degrees and all their interns have BAs. That’s a reasonably good rule of thumb in most cases.
Greg Lewis: Now, I would suggest, of course, if you’re trying to progress along that track, an advanced degree seems like an important asset to continue. I’m not going to say that it’s like a glass ceiling if you don’t have one, but the observation would suggest it’s a really important thing to have in terms of further progress. That may vary a lot depending on different areas. Maybe certain areas in the government may not require an advanced degree to do while academia typically would.
Greg Lewis: So they do vary a lot. So there’s an option value story whereby if one already has one, or if one can get one, or if one is not sure what one wants to do next and wants to keep one’s options open in terms of where one can best contribute, getting an advanced degree often does help, insofar as it won’t close off… Not easy progress but good progress in these areas.
Howie Lempel: Yeah. Do you have a strong take on if you were talking to somebody who was considering going into the area and they were still pretty flexible, maybe they’re halfway through high school, what advice would you give them?
Greg Lewis: Yeah, that’s tricky. One of the general challenges I find in trying to give career advice in this area is the usual path for existing experts is typically, I don’t want to say they fell into it by accident because that does them a great disservice, but it’s often the thing which people go into mid career or maybe later. Which does imply there should be neat shortcuts to take, rather than, “I spent 20 years being a doctor in an unrelated discipline, but I moved into this area there afterwards”.
Greg Lewis: It’s not always clear to find out what the most efficient paths are. So people who are very early on, or very pluripotent, excuse the term, what I’d probably often recommend is often led, to a large extent, by comparative advantage. So if someone’s much better at the humanities than they are at basic sciences, for example, that may suggest they should maybe not try and flog themselves getting through a science degree for example, but maybe work from a policy side, for argument’s sake.
Greg Lewis: So it’s definitely not very clear to me how I’d prioritize within GCBRs, what interventions have the greatest promise, or even what areas of interventions have the greatest promise. Which suggests this optionality/playing to your strength strategy is often a better bet, or, as far as I can tell, often seems like a better bet.
Howie Lempel: Got it. So the next question I would normally ask would be what are some positions that it would be reasonable to aim for? If you’re a bright student who just graduated from a top college, something where it’s in your tenth percentile chance, does that mean that that’s the wrong way to think about it? And instead you’re just going to have to be more flexible instead of following your comparative advantage without focusing so much on why this position seems obviously a bit better than this other one?
Greg Lewis: Yeah, that’s pretty fraught. I’m not sure of a very good general recommendation here. Perhaps what I would say is the typical model that I see, and I see people who contribute the best, or who make very good contributions, are people who typically have a home discipline which they’re very good at, and then end up applying their background in this to other areas.
Greg Lewis: It’s not that they’re ignorant about all the other things which apply, but they have an area of expertise of their own area, and then they often draw upon that to help contribute to other problems. So the advice maybe early on is to, in a sense, have a home discipline, or a home area of expertise, be that in a particular area of science or a particular area of policy or something similar to that. And then once one has that background, to then go on to deploy this. And then how one best deploys this is quite uncertain.
Greg Lewis: So one can do this in academia itself of which there’s a few examples. One can do this in maybe civil society or think tank groups, or this liminal phase between academic research groups and a think tank which many biosecurity stakeholders seem to inhabit. Then there’s obviously directly contributing in maybe science or industry, or maybe working in the government in various forms or another.
Greg Lewis: And it’s very hard to give a crisp sense of where one would end up. Though maybe I’m slightly more confident in the initial recommendation to tool up in a relevant area if it can be tilted moderately towards GCBRs, then so much the better, but principally prioritize becoming an expert in, for example, science policy and then try and look for ways to deploy that background skills to a problem, although where you end up doing this is a little bit uncertain.
Greg Lewis: It seems fairly common for people to switch contexts during their careers, so people may go into government, go in to work for someone like the WHO, and then leave it again to work in another area, and so on and so forth. So it’s very hard to give a… I’m not sure there’s a very good linear career track thing I can separate out for you.
The response of the effective altruism community to COVID-19 [02:11:42]
Howie Lempel: Before we wrap up, I saved a couple of COVID-related questions for the end of the episode. They involve some navel gazing and I’m hoping listeners who made it this far won’t mind. What’s your take on how the effective altruism community has reacted to the pandemic?
Greg Lewis: Yeah, I’m glad you asked that question, Howie. So I’ve a few things to say. I think, to be honest, the most important thing is this. If we were to give a fair accounting of all EA has done in and around this pandemic, I think this would overall end up reasonably strongly to its credit. For a few reasons. The first is that a lot of EAs I know were, excuse the term, comfortably ahead of the curve compared to most other people, especially most non-experts in recognizing this at the time: that emerging infectious disease could be a major threat to people’s health worldwide. And insofar as their responses to this were typically either going above and beyond in terms of being good citizens or trying to raise the alarm, these seem like all prosocial, good citizen things which reflect well on the community as a whole.
Greg Lewis: And I know there are some folks in this community who are contributing more directly in terms of addressing this pandemic. And I think as a community we can, to some extent, all bathe in the reflected glory in terms of the valuable work they’re doing. And I also think some of the brainstormers tended to be pretty nervy, have come up with some useful ideas and some of the projects which are being initiated or spun up or tried at the moment seem good, in expectation. It’s obviously too early to say whether they pan out but they seem like attempts worth making and are worthwhile. So all that is great. But unfortunately I’ve got more to say.
Greg Lewis: So, putting things politely, a lot of the EA discussion, activity, whatever you want to call it, has been shrouded in this miasma of obnoxious stupidity, and it’s been sufficiently aggravating for someone like me. I sort of want to consider whether I can start calling myself EA adjacent rather than EA, or find some way of distancing myself from the community as a whole. Now the thing I want to stress before I go on to explain why I feel this way is that unfortunately I’m not alone in having these sorts of reactions. Because if it was just me, people probably shouldn’t really care, despite being the guy who wrote the piece on epistemic modesty, I’m pretty arrogant, pretty unpleasant, pretty disagreeable and so it doesn’t really matter what I think.
Greg Lewis: But at least I have a few people who talk to me now, who, similar to me, have relevant knowledge, background and skills. And also, similar to me, have found this community so infuriating they need to take a break from their social media or want to rage quit the community as a whole. Now, unlike me, these people are not very irritable, very impatient, very disagreeable. In fact, if you imagine a scale, Howie, from you to me they’re like a seven or eight on that scale in terms of being in your direction. So I think there’s just a pattern whereby discussion around this has been very repulsive to people who know a lot about the subject is, I think, a course for grave concern.
Greg Lewis: That EAs approval rating seems to fall dramatically with increasing knowledge is not the pattern you typically take as a good sign from the outside view. And I remember 80K wrote a post a while ago on accidental harm, saying how people who are trying to do good can nonetheless cause accidental harm. And I feel like a lot of the issues which make these problems difficult also apply to this one. So there’s limited information. It’s very hard to interpret. You have to extrapolate or aggregate across disparate areas. You have to make decisions in haste. It’s very fast moving, and there’s a risk of large harms if you get it wrong one way or the other. And I remember recommendations there where, for example, for fields which are technical, which I think most ones related to this pandemic are, it cautioned that you might have to spend years tooling up to be in a position to help. And also, I think it mentioned things like worth: if someone’s making a decision which seems weird to someone who’s an existing stakeholder, maybe we should try and better understand why before making an alternative which you take to be a better recommendation. And I guess it seems like these lessons have not exactly always been followed to the best of everyone’s ability.
Greg Lewis: I see things like people say, “Oh, isn’t this intervention a good idea because if we compare different countries to each other, ones which did this had less epidemics”. And it’s like “Well, usually we think ecological cross country capacities are pretty dubious in terms of data”.
Greg Lewis: Or, “Oh, the epidemic slowed after country X did Y”. And it’s like, “Yes, but they’re doing an entire alphabet of other things as well”. And this general sense of just playing very fast and loose is pretty frustrating. I have experienced a few times of someone recommending X, then I go into the literature, find it’s not a very good idea, then I briefly comment going, “Hey, this thing here, that seems to be mostly ignored”, then I get some pretty facile reply and I give up and go home. And that’s happened to other people as well. So I guess given all these things, it seems like bits of the EA response were somewhat less than optimal. And I think for ways it could have been improved were mostly in the modesty direction. So, for example, I think several EAs have independently discovered for themselves things like right censoring or imperfect ascertainment or other bits of epidemiology which inform how you, for example, assess the case fatality ratio. And that’s great, but all of that was in most textbooks and maybe it’d have saved time had those been consulted first rather than doing something else instead.
Howie Lempel: Just on that one. Sorry to nitpick on one of them, but I think it’s interesting because I think there are a bunch of different complaints going on here. So for that one, it seems like they rediscovered the thing and so it didn’t lead them to get a less accurate answer. So is the problem you’re trying to solve there, you just want to help them be more efficient? Or is it that you want them to cite the right people when they start talking about right censoring and under-ascertainment? What exactly is going on there? Because it seems, at least possible to me, that an EA who’s learning about epidemiology for the first time might read an epidemiology paper and have some background in some other social science and say, “Oh yes, there’s a right censoring issue”, and now they’ve learned it. And nothing went wrong.
Greg Lewis: Yes, that’s my very long impromptu listing of [inaudible] which I think is like a few different problems. That particular problem is one of being inefficient. It doesn’t really matter how you pick up the stuff as long as you get the right information. But typically for most fields of human endeavor, we have a reasonably good way which is probably reasonably efficient in terms of picking up the relevant level of knowledge and expertise. Now, it’s less efficient if you just target it, if you know in advance what you want to know ahead. But unfortunately, this area tends to be one where it’s a background tacit knowledge thing. It’s hard to, as it were, rapier-like just stab all the things, in particular, facts you need. And if you miss some then it can be a bit tricky in terms of having good ideas thereafter.
Greg Lewis: The other problems are people often just having some fairly bad takes on lots of things. And it’s not always bad in terms of getting the wrong answer. I think some of the interventions do seem pretty ill-advised and could be known to be ill-advised if one had maybe done one’s homework slightly better. These are complicated topics generally: something you thought about for 30 minutes and wrote a Medium post about may not actually be really hitting the cutting edge. But it’s also, I think, a challenge in a sense this thing whereby getting the right belief via the right process does in fact matter. So let’s take a concrete example. So I think President Trump at the moment is suggesting that, as it were, the cure is worse than the disease with respect to suppression. And so, wouldn’t it be better if we just didn’t do so much of that. And just let the economy start running again.
Greg Lewis: Now obviously that’s a very controversial view. But suppose we’re clairvoyant and we see in two years’ time, we actually see that was right. Maybe all of the suppression doesn’t really work as we’d hoped, and maybe in the worse case, we end up suppressing for a while but give ourselves an even worse problem when it’s winter time in the Northern Hemisphere. Whereas the US, which took this early hitting and got castigated for, actually turns out to be faring much better thereafter. Say that’s true – I don’t think we can rule that out for argument’s sake.
Greg Lewis: I think very few people would be willing to, well, maybe a few people listening to this podcast can give Trump a lot of credit for calling it well. Because they would probably say, “Well yeah, maybe that was the right decision but he chose it for the wrong reasons or the wrong epistemic qualities”. And I sort of feel like a similar thing sort of often applies here. So, for example, a lot of EAs are very happy to castigate the UK government when it was more going for mitigation rather than suppression, but for reasons why, just didn’t seem to indicate they really attended to any of the relevant issues which you want to be wrestling with. And see that they got it right, but they got it right in the way that stopped clocks are right if you look at them at the right time of day. I think it’s more like an adverse rather than a positive indicator. So that’s the second thing.
Greg Lewis: And the third thing is when you don’t have much knowledge of your, perhaps, limitations and you’re willing to confidently pronounce on various things. This is, I think, somewhat annoying for people like me who maybe know slightly more as I’m probably expressing from the last five minutes of ranting at you. But moreover, it doesn’t necessarily set a good model for the rest of the EA community either. Because things I thought we were about were things like, it’s really important to think things through very carefully before doing things. A lot of your actions can have unforeseen consequences. You should really carefully weigh things up and try and make sure you understand all the relevant information before making a recommendation or making a decision.
Greg Lewis: And it still feels we’re not really doing that as much as we should be. And I was sort of hoping that EA, in an environment where there’s a lot of misinformation, lots of outrage on various social media outlets, there’s also castigation of various figures, I was hoping EA could strike a different tone from all of this and be more measured, more careful and just more better I guess, roughly speaking.
Howie Lempel: So one thing is finding examples of things that EAs did wrong; I think EAs castigating the UK government was one of the clearest and what’s the negative signal that you get from that?
Greg Lewis: Well, I think this is twofold. So one is, if you look at SAGE, which is the Scientific Advisory Group for Emergencies, who released what they had two weeks ago in terms of advice that they were giving the government, which is well worth a read. And my reading of it was essentially they were essentially weeks ahead of EA discourse in terms of all the considerations they should be weighing up. So obviously being worse than the expert group tasked to manage this is not a huge rap in terms of, “Well you’re doing worse than the leading experts in the country.” That’s fair enough. But they’re still overconfident in like, “Oh, don’t you guys realize that people might die if hospital services get overwhelmed, therefore your policy is wrong.” It seems like just a very facile way of looking at it.
Greg Lewis: But maybe the thing is first like, not having a very good view. The second would be being way too overconfident that you actually knew the right answer and they didn’t. So much that you’re willing to offer a diagnosis, for example, “Maybe the Chief Medical Officer doesn’t understand how case ascertainment works or something”. And it’s like this guy was a professor of public health in a past life. I think he probably has got that memo by now. And so on and so forth.
Howie Lempel: How often do you think that EAs were coming to wrong conclusions through this?
Greg Lewis: Yeah, that’s a good question. I think typically, in a sense when you’ve got two options, you can get it right half the time just by chance. Is X a good or a bad idea? That’s maybe a little bit cheap but that is, to some extent true. I think, as I said, I’ve always spent most of my time whining about stuff. I think, on balance, it has been good what EA has done in this area and so a typical EA activity here has been consistent social distancing, raising the alarm: all of which I think stands to its credit. I also should stress that I fear people are noticing already from this transcript that these things are probably going to particularly irritate me in particular, maybe beyond their objective merits if we’re trying to weigh things up. Hence, why I spent maybe 10 minutes about this and two minutes about all the good things they did as well.
Greg Lewis: That being said, I think there have been some instances that have been at least very dicey. So beside UK policy castigation which seems to be insensitive as to whether it’s a good or a bad idea, they’ll still get castigated in the same sort of way, and you want to have a reliable process as well as the answer, sometimes. And you want to track the truth as well. Some of the things have been quasi-antisocial prepping. So things like “I’m going to buy some medical equipment that we can expect will be scarce, or personal protective equipment, or various drugs”, which seems bad because the typical EA person is going to be pretty low risk compared to the wider population. This seems somewhat morally dubious in terms of public good provision. I think also the sort of ideas which I’ve seen thrown around are at least pretty dicey. So one, in particular, is the use of cloth masks; we should all be making cloth masks and wearing them.
Greg Lewis: And I’m not sure that’s false. I know the received view in EA land is that medical masks are pretty good for the general population which I’ll just about lean in favor of, although all of these things are uncertain. But cloth masks seem particularly risky insofar as if people aren’t sterilizing them regularly which you expect they won’t: a common thing about the public that you care about is actual use rather than perfect use. And you have this moist cloth pad which you repeatedly contaminate and apply to your face which may in fact increase your risk and may in fact even increase the risk of transmission. It’s mostly based on contact rather than based on direct droplet spreads. And now it’s not like lots of people were touting this. But lots on Twitter were saying this. They cite all the things. They seem not to highlight the RCT which cluster analyzed healthcare workers to medical masks, control, and cloth masks, and found cloth masks did worse than the control.
Greg Lewis: Then you would point out, per protocol, that most people in the controlled arm were using medical masks anyway or many of them were, so it’s hard to tell whether cloth masks were bad or medical masks were good. But it’s enough to cause concern. People who write the reviews on this are also similarly circumspect and I think they’ve actually read the literature where I think most of the EAs confidently pronouncing it’s a good idea generally haven’t. So there’s this general risk of having risky policy proposals which you could derisk, in expectation, by a lot, by carefully, as it were, checking the tape.
Howie Lempel: Yeah, so I guess I agree with you that there were some interventions going around. The antisocial prepping I think was definitely a thing that was happening. I have mixed feelings about it, in that it depends in part when you were doing it. I don’t know, I tried and then failed to get myself a mask in January, then afterwards felt I hadn’t thought through the considerations. Felt bad about that. I just think once it becomes salient that doctors desperately need masks, it’s not a good time to buy them; I buy that. I think, yes, some of the riskier ideas such as cloth masks floating around don’t necessarily seem really wise. I just don’t have an active belief that they are an ex-ante mistake, I guess: do you?
Greg Lewis: Yeah. I would be genuinely deeply uncertain whether mass public administration or mass public use of cloth masks help or harm. It’s not like, “Oh it might be useless, but would hate to roll the dice anyway.” It’s more like, “Well, actually this could be PlayPumps Mark II Pandemic Edition” in terms of, “Oh, there’s things that sort of make sense but there’s lots of things where it could go wrong, and isn’t really crisp either way. Very equivocal. Doesn’t look great, but we’re going to try anyway”. Now, you could go, “Well, we just sort of pick on EV grounds”, and that’s fair enough. Well my EV is pretty close to zero. It’s not clear what the sign is. And I still think if you’re going to do this, or you’re going to make your recommendations based on expectation, you should be checking very carefully to make sure your expectation is as accurate as it could be, especially if there’s like a credible risk of causing harm and that’s hard to do for anyone, for anything. I mean cf. the history of GiveWell, for example, amongst all its careful evaluation. And we’re sort of at the other end of the scale here. And I think that could be improved. If it was someone like, “Oh, I did my assessment review of mask use and here’s my interpretation. I talked to these authors about these things or whatever else”, then I’d be more inclined to be happy. But where there’s dozens of ideas being pinged around… Many of them are at least dubious, if not downright worrying, then I’m not sure I’m seeing really EA live out its values and be a beacon of light in the darkness of irrationality. Now again, maybe I’m just too disagreeable or maybe I have overly high standards or something else.
The response of 80,000 Hours to COVID-19 [02:28:12]
Howie Lempel: So this is something that 80K, I think, participated in. We did two episodes of the podcast that were just me and Rob who are not experts saying what we knew at the time about the epidemic. We’ve done a bunch of content on COVID. I’m curious how you feel about that and whether there are mistakes that you think that we are making?
Greg Lewis: Sure. The direction I would be keen for EAs to go in is essentially paying closer attention to available evidence such as it is. And there are some things out there which can often be looked at or looked up, or existing knowledge one can get better acquainted with to help inform what you think might be good or bad ideas. And I think, also, maybe there’s a possibility that places like 80K could have a comparative advantage in terms of elicitation or distillation of this in a fast moving environment, but maybe it’s better done by, as it were, relaying on what people who do this all day long, and who have a relevant background are saying about this. So yeah, maybe Marc Lipsitch wants to come on the 80K podcast, maybe someone like Adam Kucharski would like to come on. Or like Rosalind Eggo or other people like this. Maybe they’d welcome a chance of being able to set the record straight given like two hours to talk about their thing rather than like a 15 minute media segment. And it seems like that might be a better way of generally improving the epistemic waterline of EA discussions, rather than lots of people pandemic blogging, roughly speaking, and a very rapid, high turnaround. By necessity, there’s like limited time to gather relevant facts and information.
Howie Lempel: Yeah, that’s useful. What’s the answer there? It’s like having either Lipsitch or Kucharski on the podcast would be great. Would be concerned about wasting their time. Like Rob and I are just going to be unusually low cost. And so the question is, it’s like an extra podcast instead of trading off on anything. Yeah. It’s not obvious to me that we should have done them, but they’re pretty low cost and so like the correct question is like did this do harm?
Greg Lewis: Yeah. I don’t think it did much harm. Like the podcasts I remember, like Cassidy’s I think was very good, for example. The other podcasts, I think, were fine. It probably didn’t cause harm but the general point, Howie, genuinely is this. A lot of people, well one of the things I’m worried about, it’s like a lot of people are going to look at COVID-19, start want get involved in GCBRs. And sort of all these people are cautious, circumspect, lot’s of discretion and stuff like that. I don’t think 80Ks activity on this has really modeled a lot of that to them. Rob, in particular, but not alone. So having a pile of that does not fill me with great amounts of joy or anticipation but rather some degree of worry.
Greg Lewis: I think that does actually apply even in first order terms to the COVID-19 pandemic, where I can imagine a slightly more circumspect or cautious version of 80K, or 80K staff or whatever, would have perhaps had maybe less activity on COVID, but maybe slightly higher quality activity on COVID and that might’ve been better. But anyway, I mean I’m loading quite a lot on EA social media activity rather than what people did as part of their orgs; maybe that’s unfair. But that’s the general vibe I got.
Howie Lempel: Cool. That’s helpful.
Greg Lewis: I mean people like me are very hesitant to talk very much on COVID for fear of being wrong or making mistakes. And I think that fear should be more widespread and maybe more severe for folks who don’t have the relevant background who’re trying to navigate the issue as well.
Howie Lempel: Yeah, I actually don’t know what direction I think that that goes in.
Greg Lewis: I sort of get the impression, Howie, to be honest, that a lot of you guys are just tilted off the face of the planet by COVID-19. And I get it, but I still feel I want EAs to be like Kipling in that we keep our heads while all around are losing theirs rather than, “Oh, I’m obsessed by COVID and just do work on it because I’m scared” or something. Yeah, I definitely appreciate it. Like I’m worried too. But I sort of want EA to be reasonably cool-headed about doing things and this hasn’t always happened.
Howie Lempel: Yeah, I buy that. Yeah, so I think it was really helpful to get all of that feedback and criticism and I think that I have already found criticism from Greg on this and related issues to be personally valuable and make me sort of reflect on how I’ve engaged with the epidemic but I think it is worth keeping in mind Greg’s previous “All things considered” statement that he does believe that EA, on the whole has been net positive during the events. So Greg, I’m curious if that still seems true to you now that you’ve listed out the gripes and if so, what are some of the positives?
Greg Lewis: Yeah, sure. I mean it definitely seems true. In fact, I get slightly more embarrassed on reflection by how much time I spent on these things relative to their actual relative importance. However, that being said… So as I mentioned, I mean EA’s doing a lot of good things with respect to this and hopefully more generally. So as mentioned, they were ahead of the curve in noticing it’s a problem. They generally reacted to this and, by and large, prosocial ways with exceptions I noted before. But the general trend is definitely in the positive direction. Typically much better than most other groups or communities of people did. I think there are also people, I may join them at some stage, who are in the community and are also contributing to mitigating this pandemic. And I think they’re doing extremely valuable work and adding a lot of value. And now, it’s not the case that I can take credit for them.
Greg Lewis: But I think as a community we can maybe take credit for, in some indirect sense, having people like that within it, which I think stands to our credit. So on balance, good, but obviously not optimal.
Howie Lempel: So, in addition to the work that you actually get paid to do, I feel like once every six months or so we get a new Greg Lewis blog post. Is there anything in the pipeline that we can expect to see sometime soon?
Greg Lewis: Yes, there is. I have noticed, of course, the irony of me preaching various things which I then fail miserably to practice myself, but no matter. So a couple of the ideas I’m working on, in my typical oeuvre of being edgy on the internet, is I have a piece mostly done with a suitably non-inflammatory title called “Contra Cause X”.
Greg Lewis: So this is essentially suggesting that if we look at our track record so far, the likelihood of finding a major new cause area of the scale of like global health, animal welfare, is very unlikely, by just observing the track record so far. And then more edgily going onto just, “Oh no, we’ve basically solved this problem. So we basically have identified all the main important cause areas of our age, and so now it’s figuring out the mid-level tactical details of how best to contribute”.
Greg Lewis: Yeah, I mean that’s provocative; who knows if it’s true? But maybe it’ll be interesting. The other one I have… I’m not a philosopher, although I’ve allegedly written a piece on epistemic modesty, it doesn’t stop me attempting to do philosophy every once in a while.
Greg Lewis: So some folks at my sister institute, the Global Priorities Institute, have been doing various works on how one accounts for or deals with great uncertainty exploring these under the heading of cluelessness, or complex or consequentialist cluelessness. And so despite not being a philosopher I thought, “Oh, I can write something about this”. So I have. It’s essentially trying to argue the “naive, orthodox, Bayesian, just take the expected value approach” is basically fine. We should just do that. None of this complicated imprecise credences stuff: don’t worry about that.
Greg Lewis: I then plagiarize folks like Amanda Askell who suggest that maybe we should use credo-resilience: so how fragile, in essence… How much your credence has changed, is a better way of trying to account for radical uncertainty than represented by other measures of credal resilience. So there’s something else which I’ve also mostly finished, which I may subject the wider internet to at some stage in the future.
Howie Lempel: Well looking forward to getting to read all of the stuff coming down the pipeline, and really appreciate you coming on the show.
Greg Lewis: Thanks so much for having me. It’s a pleasure to be on here.
Rob’s outro [02:36:22]
Robert Wiblin: I hope you enjoyed that conversation between Howie and Greg.
I’m personally going to keep working on COVID-19 for a little while longer, but I’m happy to see the rest of the team getting back to focusing on some of the more neglected and unappreciated problems in the world.
Just a reminder that if you want to read more about COVID-19, the 80,000 Hours team has produced a fantastic package of 10 pieces about how to stop the pandemic. You can find those at 80000hours.org/covid-19/.
If you want to learn more about GCBRs, you should definitely check out the profile of global catastrophic biological risks that Greg wrote for 80,000 Hours. You can find that at 80000hours.org/problem-profiles/global-catastrophic-biological-risks/
The 80,000 Hours Podcast is produced by Keiran Harris. Audio mastering by Ben Cordell. Transcripts by Zakee Ulhaq.
Thanks for joining, talk to you in a week or two.
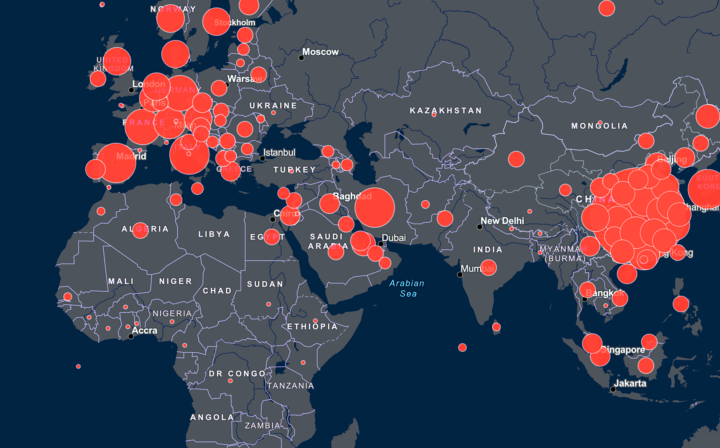




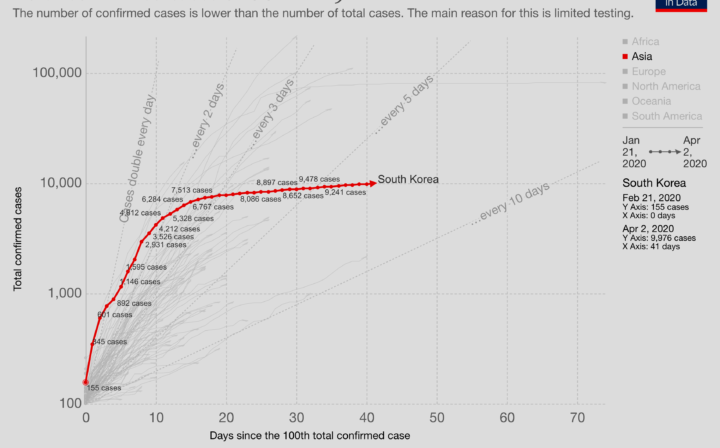
Related episodes
About the show
The 80,000 Hours Podcast features unusually in-depth conversations about the world's most pressing problems and how you can use your career to solve them. We invite guests pursuing a wide range of career paths — from academics and activists to entrepreneurs and policymakers — to analyse the case for and against working on different issues and which approaches are best for solving them.
Get in touch with feedback or guest suggestions by emailing [email protected].
Our crash course on transformative AI
We've carefully selected 10 key episodes to help listeners get to grips with the potential upsides and downsides of powerful, transformative AI.
Check out 'The 80,000 Hours Podcast on AI'
Listen here, or anywhere you get podcasts:
If you're new, see the podcast homepage for ideas on where to start, or browse our full episode archive.